I’m always looking for collaborators for future experiments. If you’re interested in collaborating on scientifically rigorous self-experiments with low-carb foods, supplements, or other health interventions, please let me know in the comments or via the contact form on the right.
I finally finished and posted my flour replacement tests. This was a really fun experiment. I found a number of alternate flours with low BG impact that I hadn’t heard of before (e.g. ground chia seed and King Arthur Keto blend) and learned a lot about the behavior and exact BG impact of the flours I had been using. This has got me interested in doing some low-carb baking experiments again. I’m going to try making pizza first and will report back if anything works well.
Food effect: next week is Thanksgiving here in the US, so I’ll be doing less food effect tests, but I should be able to fit in a few more whole foods.
Blood pressure:
I’ll be continuing the deep breathing study, but it will take another 3 weeks to finish and analyze.
I’m going to take advantage of the holiday to do try tracking my BP over the course of a day to see how it varies. I’ll post that data sometime in the next couple weeks.
On the allergy study, I’ll be finishing the last antihistamine run, unblinding, and analyzing the data, so I should get that posted next weekend.
– QD
Active & Planned Experiments
Blood Glucose Impact of Low-Carb Foods & Ingredients
Goal: Determine blood glucose impact of low-carb foods and ingredients
Historically, there hasn’t been a lot of low-carb replacements for flour available, mostly almond flour, coconut flour, and resistant starches. Similar to other low-carb products, a ton of new flour replacements have hit the market in the last few years. As always, the net carb counts look good, but I wanted to test them to see if they really hold up (see evidence of blood glucose impact of dietary fibers here & here).
Between my own searching and reader recommendations (1, 2, 3), Foods. I tested 18 flours from 6 different categories (grouped by main ingredient). Here’s my overall conclusions:
Most Similar to Wheat Flour: Carbalose
<30% BG impact of wheat flour, <20% of white bread
texture & water uptake very similar to wheat flour
Lowest BG impact: Ground chia seeds
12% of wheat flour, 8% of white bread
Best Binders: Gluten, chia seeds, flaxseed, and psyllium husk
These work great to tune the texture of other flour replacements
Which one is best to use probably depends on the specific recipe/desired texture
Best Pre-made Blends: King Arthur Keto Flour & Carbquik
King Arthur is a flour substitute, though more elastic/chewy
Carbquik is like Bisquik and great for biscuits, pancakes, muffins, and other airy baked goods.
I’m always looking for collaborators for future experiments. If you’re interested in collaborating on scientifically rigorous self-experiments with low-carb foods, supplements, or other health interventions, please let me know in the comments or via the contact form on the right.
For the blood pressure and rhinitis, I’m excited to branch out to experiments other than blood glucose effects. Experiments for both will start Monday and I should have results to report in 3-4 weeks.
Experiments the past two weeks were focused finishing up the flour replacement tests. I’ve finally got that done and will be posting the results next week. In the meantime, I’ve gotten started on the whole food testing with almonds, salmon, and tuna. I’ve also done a few rounds of the vinegar tests with my standard breakfast, though that will take a decent size dataset before I’ll be able to draw any conclusions (BG on morning meals is noisy due to the dawn phenomenon).
Next week, I’ll be continuing the whole food testing and starting the blood-pressure and rhinitis experiments.
– QD
Active & Planned Experiments
Blood Glucose Impact of Low-Carb Foods & Ingredients
Goal: Determine blood glucose impact of low-carb foods and ingredients
In a previous post, I mentioned that I get a runny nose when I go for a walk in the mornings or a run in the evening. It’s not terrible, but is annoying and prevents me from breathing comfortably through my nose. I hypothesized that this was caused by allergies and proposed some experiments to check whether this was the case.
I got great feedback on that post, both from Reddit and the Quantified Self forum. In particular, several commenters suggested:
Making sure the experiments could distinguish between cold & allergens as the cause
Testing indoor exercise & no exercise in the same outdoor locations
Using an N95 mask as an alternative to allergy medicine as means of assessing whether allergens are the cause
Keeping track of weather and pollen counts during the experiment as potential confounders
Following up on these suggestions, I did a few quick experiments to narrow down what might be going on:
I sat outside, not exercising, in the same location I take my morning walk. After 1h, I did not get a runny nose. I then started walking and developed a runny nose within 15 min. (the same intensity as has occurred every day since I’ve started monitoring).
I used a rowing machine to exercise indoors at maximum intensity for 30 min., the same as my evening run. I did not develop a runny nose.
Based on these two observations and the fact that I’ve consistently gotten a runny nose on my morning walks for at least 3 weeks, it seems like the cause has to be either allergies or cold and exacerbated by physical activity.
To test the two hypotheses, I will run the following experiments:
Test 1: Walk while wearing an N95 mask both with and without the particulate filter.
The experiment will be randomized and blinded by having another person load/remove the filter
I will run 2 tests for each condition, recording whether or not I get a runny nose and it’s severity.
If I get the runny nose without the filter, but not with it, that strongly suggests the cause is allergies. If both conditions prevent a runny nose, that suggests the cause is temperature.
Test 2: Exercise (walk & run) after taking allergy medication
Take fast-acting allergy medication or a placebo 1 hour before exercising.
The experiment will be randomized and blinded by placing the pills inside of opaque gel caps and have another person randomize the treatment days for me.
If no effect is observed, take long-acting allergy medication or a placebo on alternating weeks.
I will run 3 tests for each condition, recording whether or not I get a runny nose and it’s severity.
During all experiments, I will record temperature, pollen count, and other notable weather conditions. If it is raining or unusually windy (very uncommon where I live), I will postpone the experiment to the next day.
These experiments will start next weekend, so I expect to have results to share in 3-4 weeks.
Previously, I proposed some analyses and breathing experiments to try to identify potential causes for and ways to reduce my high blood pressure. I got great feedback on that post (thanks everyone!) and have also done some preliminary breathing experiments. Based on that, I’ve finalized my experimental and analytical approach and am ready to start. This post will serve as the pre-registration of the experiments.
Details
Purpose
To identify environmental or controllable factors that have a significant impact on my blood pressure.
To quantify the effect of known interventions for reducing blood pressure.
To find a set of interventions that enable me to reduce my blood pressure below 120/80 mmHg.
Background
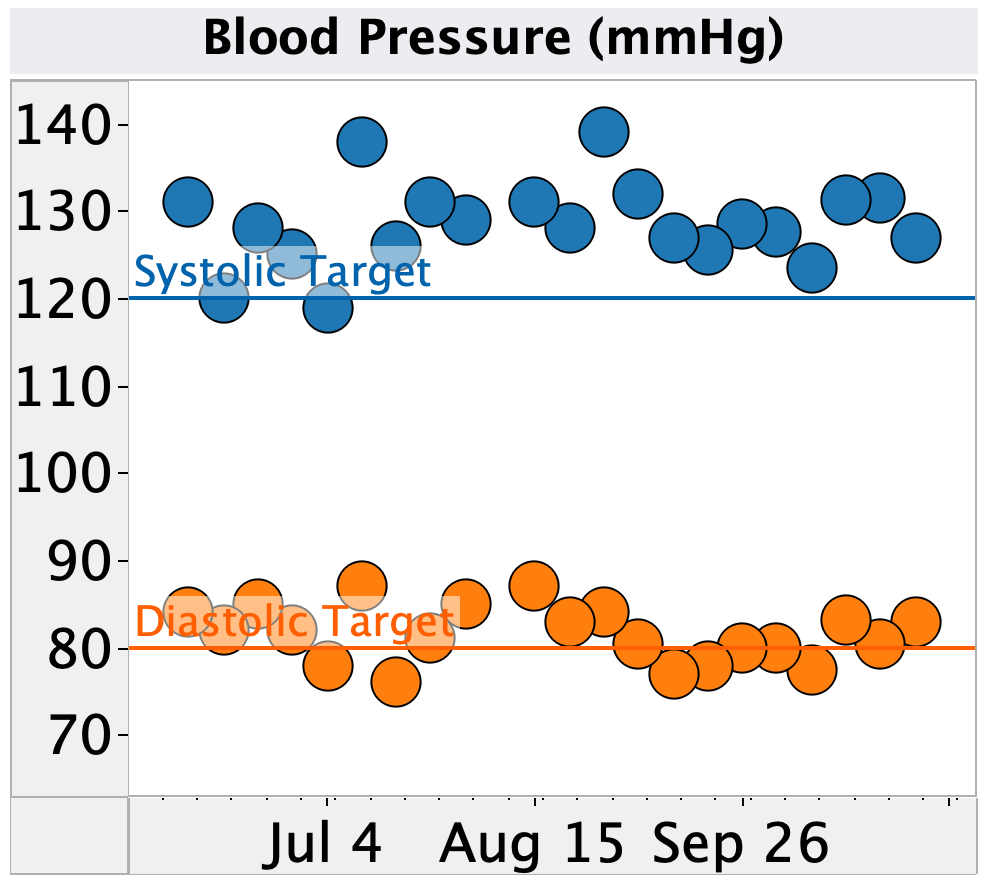
Figure 1. Weekly average of blood pressure as measured by Omron home blood pressure monitors.
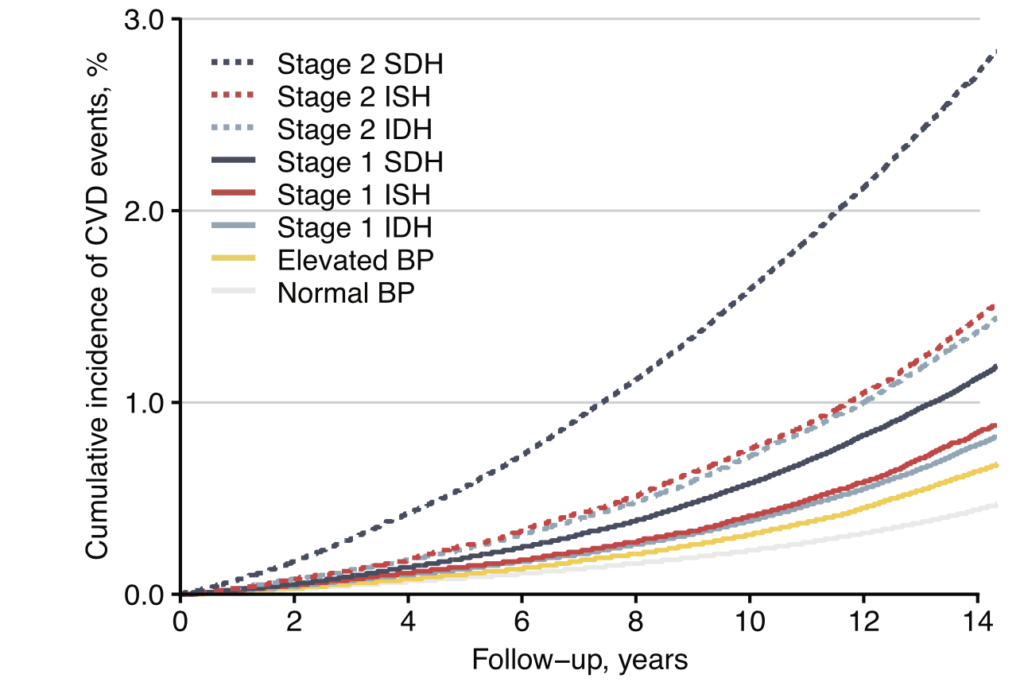
Figure 2. Cumulative incidence of cardiovascular disease vs. time for different blood pressure groups from a study of the South Korean nationwide health screening database (6.4M participants).
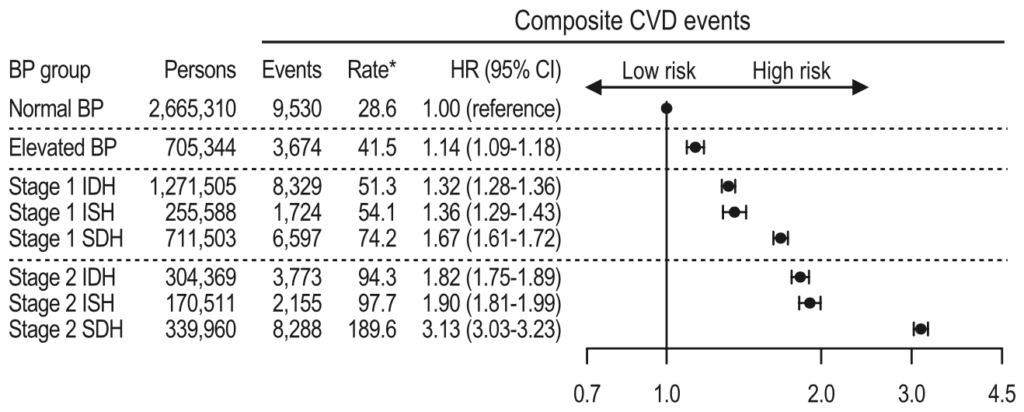
Table 1. Rate of cardiovascular disease for different blood pressure groups from a study of the South Korean nationwide health screening database (6.4M participants).
Given this, I’d like to see if I can reduce my blood pressure and reduce the strain on my heart and circulatory system.
There are numerous medications that lower blood pressure, but all risk of side effects. Before I pursue that route, I’d like to better understand the cause of my elevated blood pressure and see if any diet or lifestyle interventions can ameliorate it.
As mentioned above, I’ve been measuring my blood pressure for the past 4 months, along with blood glucose, sleep, weight, and exercise. This provides a (hopefully) rich dataset for identifying environmental or lifestyle factors that influence my blood pressure. Notably, I’ve noticed that my blood pressure is elevated on days after I’ve had low blood sugar the night before, indicating a possible effect (no statistical analysis done).
As a quick test of this approach, I did one-off tests of 7 different breathing protocols. I tested one each morning after arriving at work, measuring my blood pressure before and after the protocol. I used the app iBreathe to help regulate my breathing. The results are shown below.
Change in blood pressure following different breathing protocols. Protocols descriptors are Inhale Time (s)/Hold Time (s)/Exhale Time (s)/Hold Time (s), Total Duration (min.).
With the exception of one protocol (8s inhale/8s exhale for 5 min.), I did not see a significant drop in blood pressure. However, I saw a large rise in blood pressure (+7/+3 mmHg) when I did not use a breathing protocol. Given this, I think a more extensive experimental test, focused on the longer inhale/exhale time is worth trying.
Proposed Experiments
Phase 1: Identify Potential Causes of Elevated Blood Pressure from Existing Self-Tracking Data
Data
Blood pressure:
systolic and diastolic blood pressure
Measured by Omron Evolve
Glucose:
Same day: fasting BG
Previous day: average BG, time low (70, 60, & 50), time high (120, 140, 160), & coefficient of variation
Previous evening (after 7p): same as previous day
Measured by Dexcom G6
Sleep:
Time asleep, number of wake-ups, early rising (time woke before alarm)
Measured manually and by Apple Watch (less reliable but more data)
Other heart markers:
pulse (sleeping, morning, and awake), heart rate variability
Type of exercise the previous day (aerobic vs. strength training) and frequency of aerobic exercise
Manually recorded
Analysis
A mixed effect model will be used to calculate the effect size, standard error, 95% CI, and p-value for the correlation between each metric and systolic and diastolic blood pressure
Effects will be of significant magnitude if a reduction of 5 mmHg can be achieved via a practical variation in the correlating metric.
Given the large number of metrics being looked at, I will use p-value thresholds of:
0.02 for planning testing interventions
0.05 for follow up experiments to confirm the correlation
0.1 for further monitoring/assessment as I get more data
Phase 2: Testing Deep Breathing to Lower Blood Pressure
Background
Numerous studies, reviews, and meta-analyses have shown deep breathing to lower blood pressure in both the short and long-term (example 1, example 2).
Effect sizes are moderate (3-5 mmHg) and statistically significant for large patient populations (>10,000 patients in some studies).
Numerous breathing protocols have been tested, with varying results.
My own quick tests (see above) suggest a possible effect.
Approach
Measure blood pressure and pulse before & after the following protocols:
8s inhale, 8s exhale
Normal breathing (read and do not use app to regulate
Normal activity
Each protocol will be tested for 5 & 15 min.
Each protocol/time combination will be measured five times.
Conduct measurements 1/day in the mornings.
If any protocols show significant reduction in blood pressure (>3 mmHg), optimize the protocol and design/execute an experiment to test the long term effect.
Measurement
Blood pressure and pulse will be measured with an Omron Evolve.
Analysis
Student’s t-test will be used to test if the blood pressure change for any of the protocols is different from that of normal breathing.
These experiments will start this week, so I expect to have results to share in ~4 weeks.