Disclaimer: This experiment was only done on one person (myself) and is not fully randomized, placebo controlled, or blinded. Please take all conclusions with the appropriate skepticism.
Summary
Vitamin C is reported to falsely raise blood glucose readings in both fingerstick and continuous glucometers. I wanted to know if this was something that I (and others) should be concerned about, but all the reports I found were for intravenous vitamin C and I couldn’t get any data from the CGM companies.
To get an answer, I tested it myself, monitoring blood glucose after ingesting 2-6g of vitamin C, 20-60 the FDA recommended daily amount (but known to be safe). I did not observe any consistent or sustained increase in blood glucose, so I conclude that ingested vitamin C has no measurable impact on my blood glucose measurements at any practical quantity.
Details
Background
When I first tried out the FreeStyle Libre CGM, I read through the manual and noticed an unusual warning:
Vitamin C is an essential nutrient and present in tons of foods and most multivitamins. If it falsely raises glucose readings, that’s a huge flaw in the device.
I tried contacting Abbot, who confirmed that vitamin C can cause erroneously high glucose readings, but couldn’t point me to any studies or say how strong the effect was. I also contacted Dexcom and there support rep. said that “Vitamin C was not contraindicated for Dexcom CGMs,” but again couldn’t point me to any studies or say if they had or hadn’t run any tests.
Having failed at getting useful info directly from the CGM companies, I turned to the published literature. I found a number of reports of Vitamin C leading to high blood glucose readings (1, 2, 3, 4, 5; not exhaustive, there are many more). From these, I learned the following:
All reports in scientific or medical journals were for patients taking intravenous vitamin C.
Vitamin C can be oxidized by glucose oxidase and glucose dehydrogenase, the enzymes used to detect glucose in most portable glucometers, including most fingerstick meters and both the FreeStyle Libre and Dexcom CGMs
The increase in reported blood glucose can be extremely large; in one case a women read 343 mg/dL on standard glucometer, while a blood test showed her actual blood glucose as 49 mg/dL.
The blood levels of vitamin C in these reports were extremely high, 1,000 – 5,000 µmol/L. This is much higher than the 100-200 µmol/L observed with regular oral vitamins.
There’s only one anecdotal report on a diabetes forum of someone who saw high CGM readings after taking oral vitamin C, with numerous comments from people claiming that they do not see this.
Given all this, it seemed unlikely that regular consumption of vitamin C would significantly affect blood glucose readings, but I was left with two questions:
Was there any measurable effect of ingested vitamin C, even if small?
mega-doses of vitamin C were advocated by Linus Pauling (nobel prize winner in chemistry). His theory has since been debunked, but is unfortunately still used by many people.
Since I couldn’t find any direct studies of the effect of ingested vitamin C, I decided to do my own experiment.
Purpose
To quantify the effect of ingestion of vitamin C in blood glucose readings from Dexcom G6 and Freestyle Libre CGMs.
Design/Methods
Procedure. At selected times of day, 2, 4, or 6g of vitamin C was ingested and blood glucose monitored using a continuous glucose monitor.
Measurements. Blood glucose was measured using a Dexcom G6 CGM and FreeStyle Libre 14 day CGM.
Data Processing & Visualization. Data was visualized using Tableau.
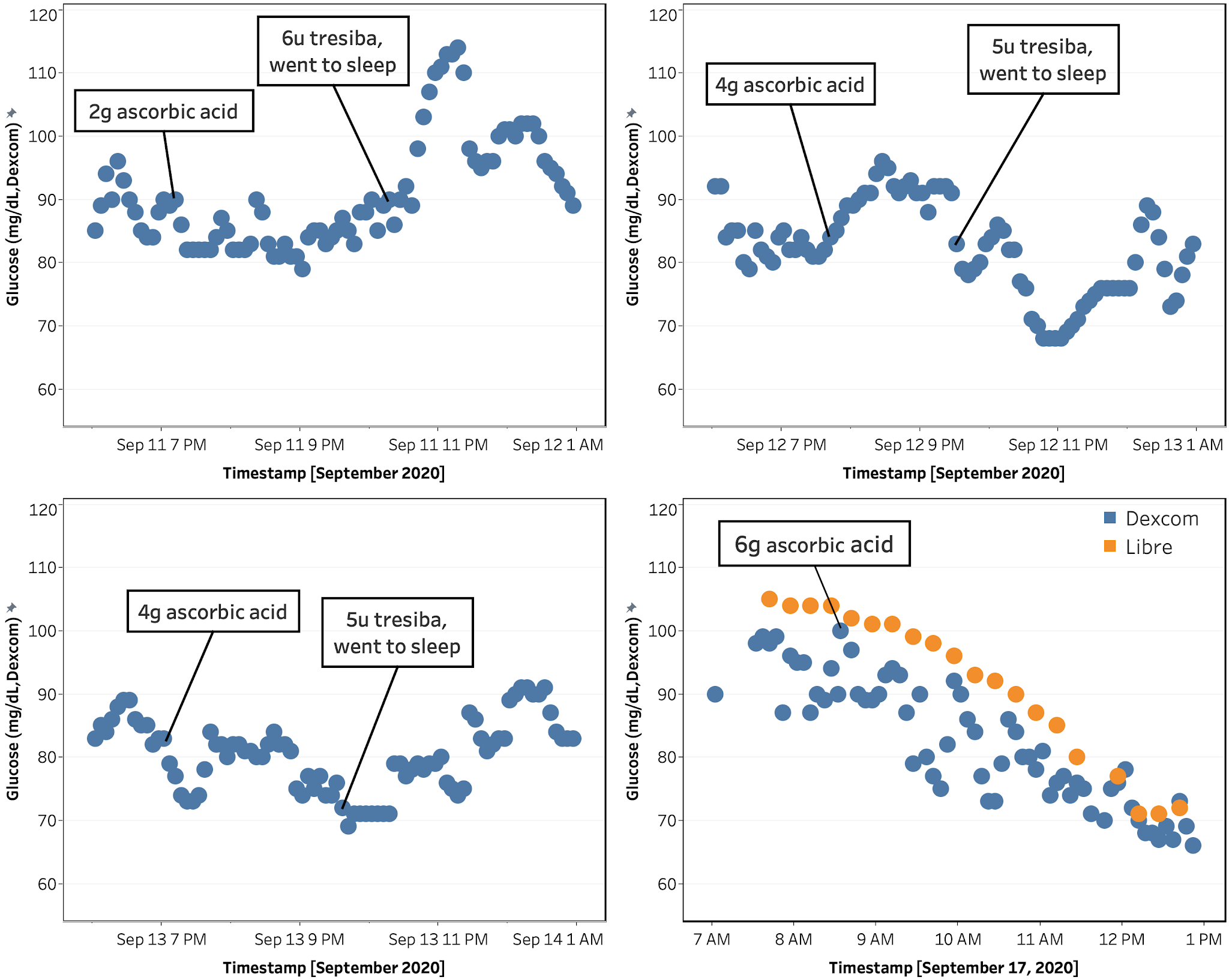
Figure 1. Blood Glucose vs. time for each of four vitamin C ingestion experiments. Color represents data from Dexcom G6 (blue) and FreeStyle Libre (orange)
According to the NIH, the recommended amount of vitamin C is 65-90 mg/day and the tolerable upper limit is 2,000 mg/day. However, studies have shown no serious adverse effects at much higher amounts and >10,000 mg/day is prescribed for treatment of certain cancers with no ill effects. Given that information, I tested ingestion of 2,000, 4,000, and 6,000 mg of vitamin C.
As can be seen in Figure 1, there was no significant rise in measured blood glucose in any of the four experiments that could be attributed to vitamin C intake. While here were transient increases in measured blood glucose in the first three measurements, they were not consistent in time or magnitude. In addition, all the reports of increases from intravenous vitamin C indicated that the effect was of long-duration (such that measured blood glucose was still elevated well after the patient arrived at the hospital or clinic).
Based on this data and the fact that typical vitamin C consumption is much less than what I took in these experiments, I conclude that ingested vitamin C has no measurable impact on blood glucose measurements at any practical quantity.
Final Thoughts & Next Experiments
This was a very satisfying experiment. Pretty quick, answered a question I wasn’t able to find in the literature or from the CGM companies (though they probably knew the answer), and results were very clear.
Next up:
Re-tune basal and bolus (meal) insulin doses
My routine has changed a lot due to working from home, changing doctors, and changing medication (due to insurance requirements). Plus, I was able to get a Dexcom G6 CGM, which is showing accuracy comparable to my blood glucose meter. Blood sugars are still good, but I think I can get them better.
This is going pretty well. As I expected, I had my basal:bolus ratio off. I’m steadily getting it corrected and it’s making my blood sugar a lot more stable.
Re-measure blood sugar impact of glucose and insulin; compare to previous data
While working from home, I’ve gained some weight (and hopefully muscle). This has resulted in a change in my insulin sensitivity. Not huge, but I need to remeasure to have an accurate baseline for future experiments.
Test the effect of some dietary supplements that have been reported to affect blood sugar in the literature, but where data insufficient or contradictory
Glutamate (reported to reduce post-prandial glucose, but magnitude and timing vary widely)
Others tbd.
As always, if you have any questions, comments, suggestions, or are interested in joining in future experiments, please let me know in the comments or send a PM via the contact form or to quantifieddiabetes_at_gmail.com.
Since I started self-experimenting to better manage my diabetes, one of the things I was most interested in was the effect of different foods on blood sugar. I follow a low-carb/keto diet and I was particularly interested in confirming if low-carb flour and sugar replacements (e.g. oat-fiber, inulin, allulose, etc.) really have as little impact as claimed.
When I first tried this, I added ingredients to my normal meals measured the change in my normal BG trends. This proved too noisy and I couldn’t get a clean measure of the effect of even pure glucose in a reasonable number of measurements (design, results).
For these experiments, I isolated the effect of the ingredient being tested by fasting for 17 h before eating/drinking. This worked really well and I was able to get reliable measurements and some (hopefully) interesting insights.
I hope some people find this interesting. If you have any questions, comments, or suggestions for future experiments, I’d love to know.
Lastly, if you’re interested in joining in any future experiments, let me know in the comments or send a via the contact form or to quantifieddiabetes_at_gmail.com.
Results for ingredients without links are in this post.
Key results
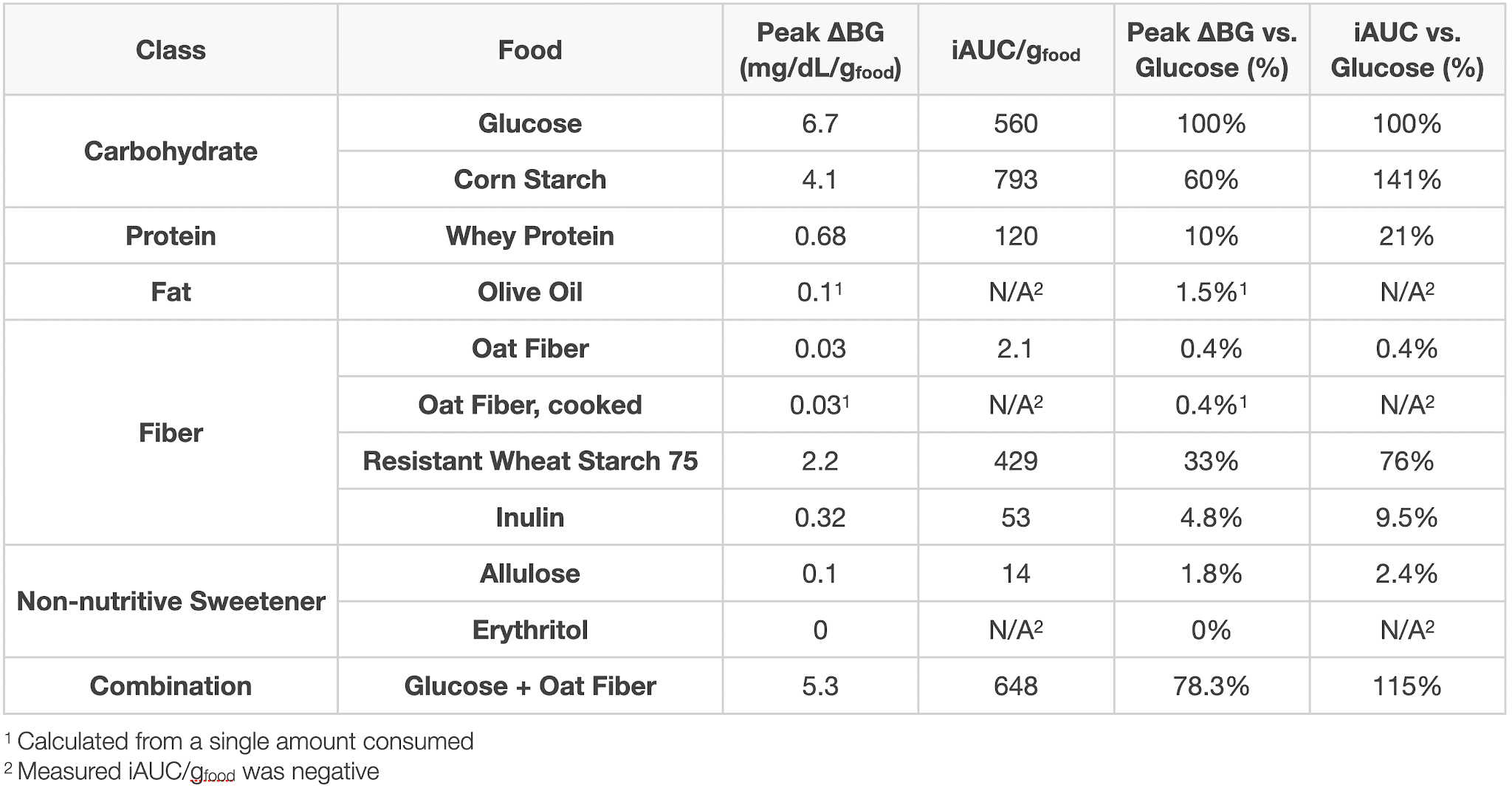
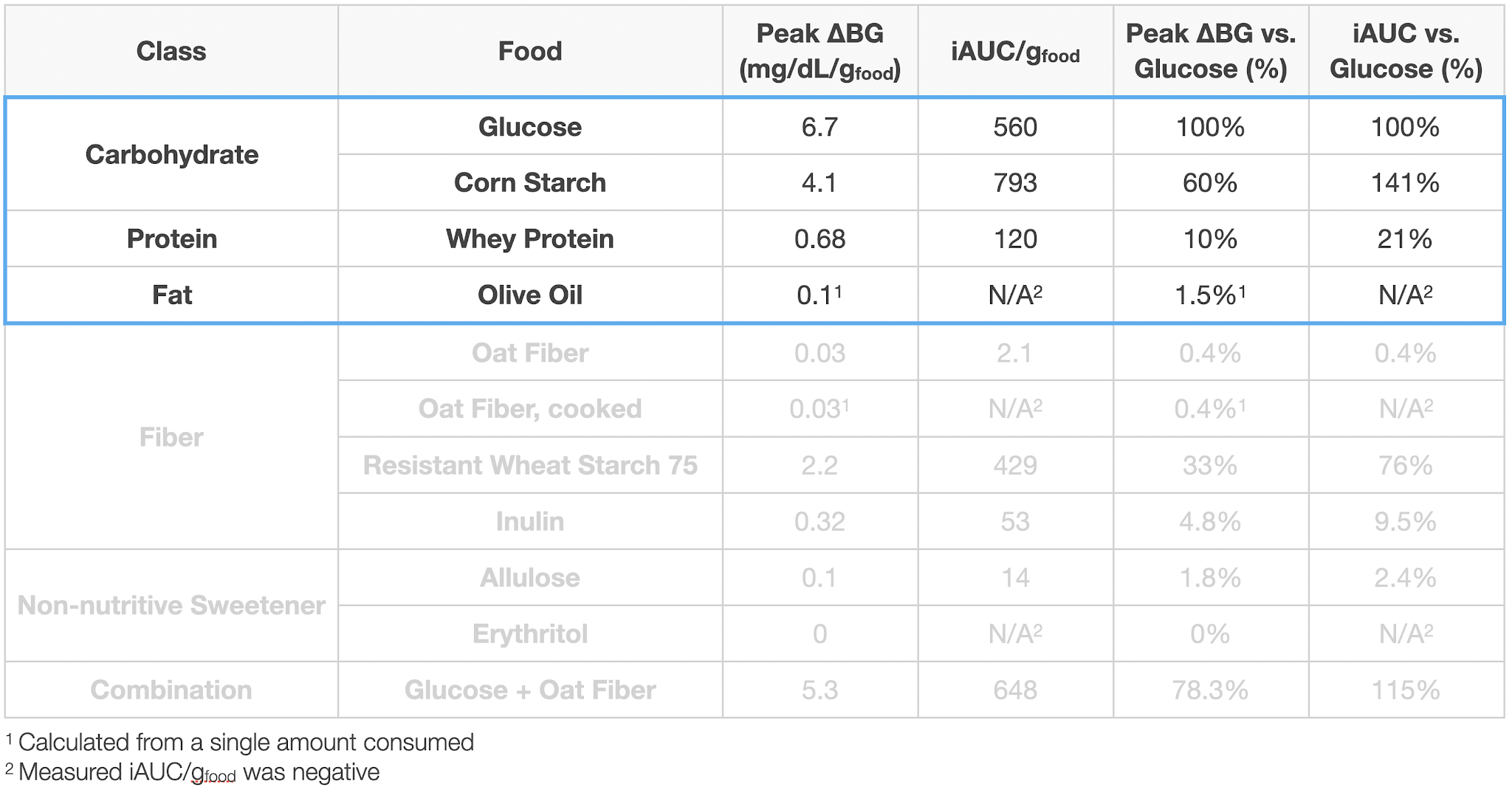
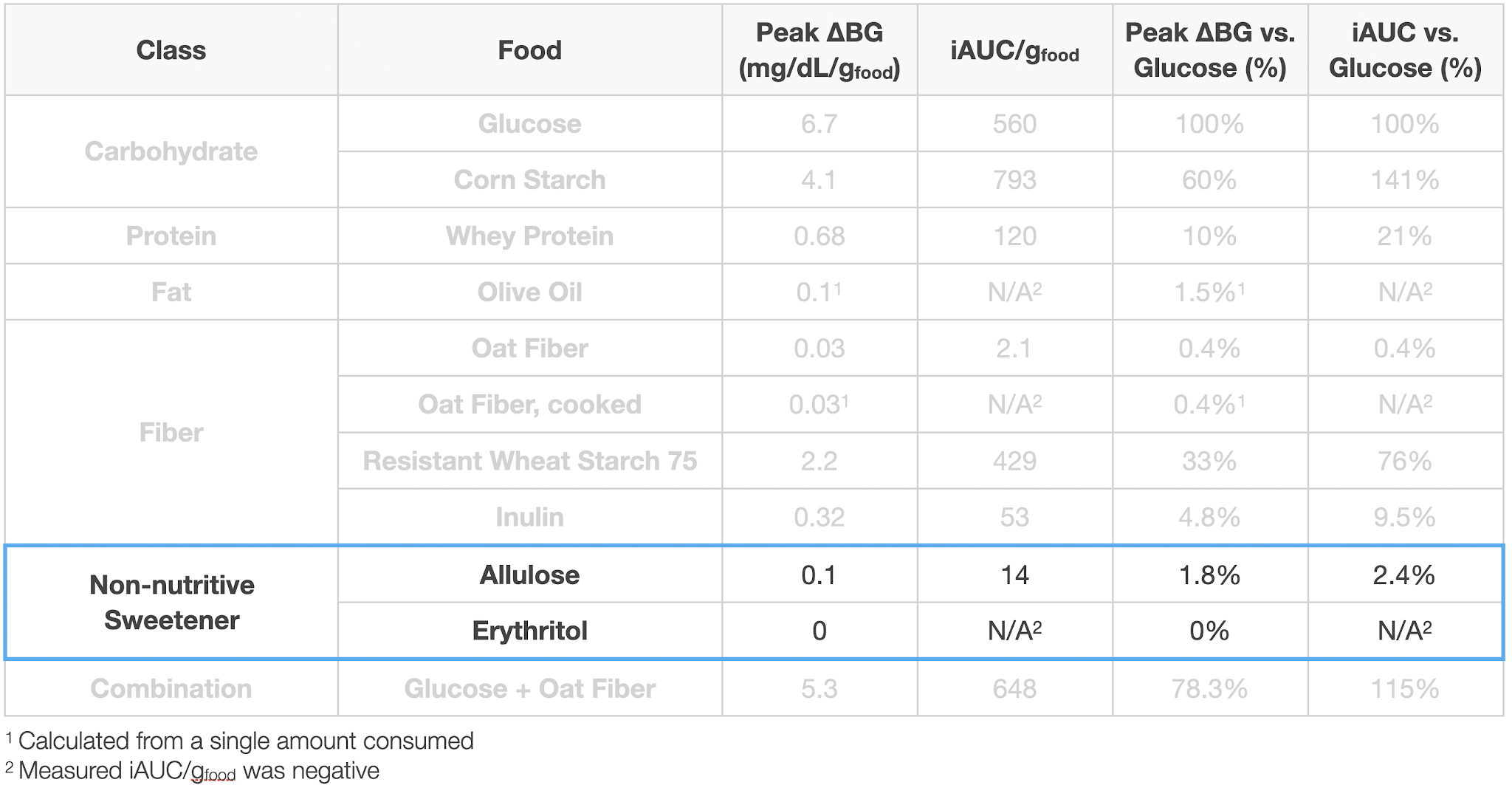
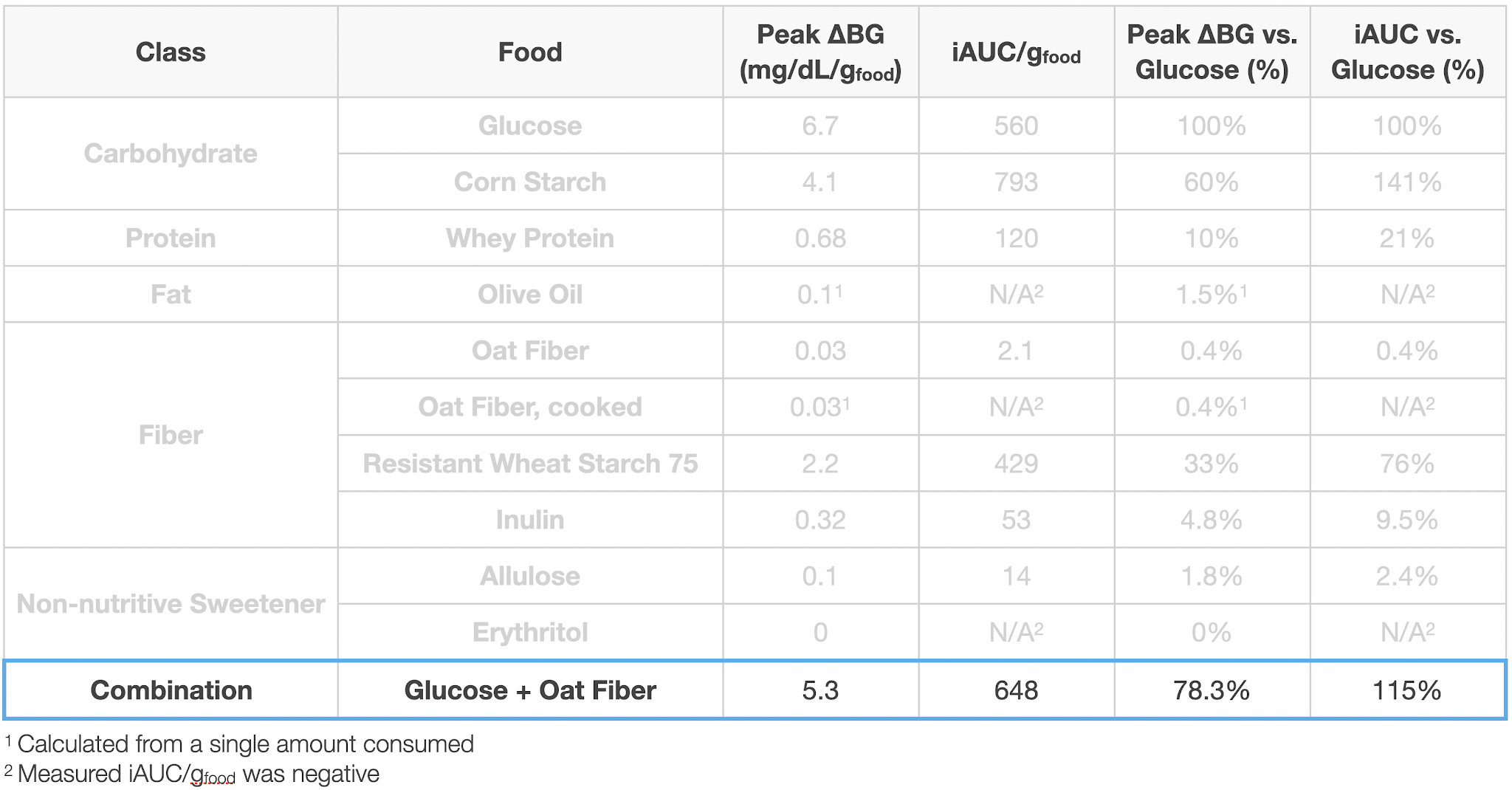
The main macronutrients, carbohydrates, protein, and fat have the expected impact. Notably:
Contrary to some claims I’ve read, fat had virtually zero impact on my blood sugar.
Starch and glucose had nearly the same impact, though slightly delayed in time. This suggests that for purposes of carbohydrate counting, I can treat all digestible carbohydrates the same.
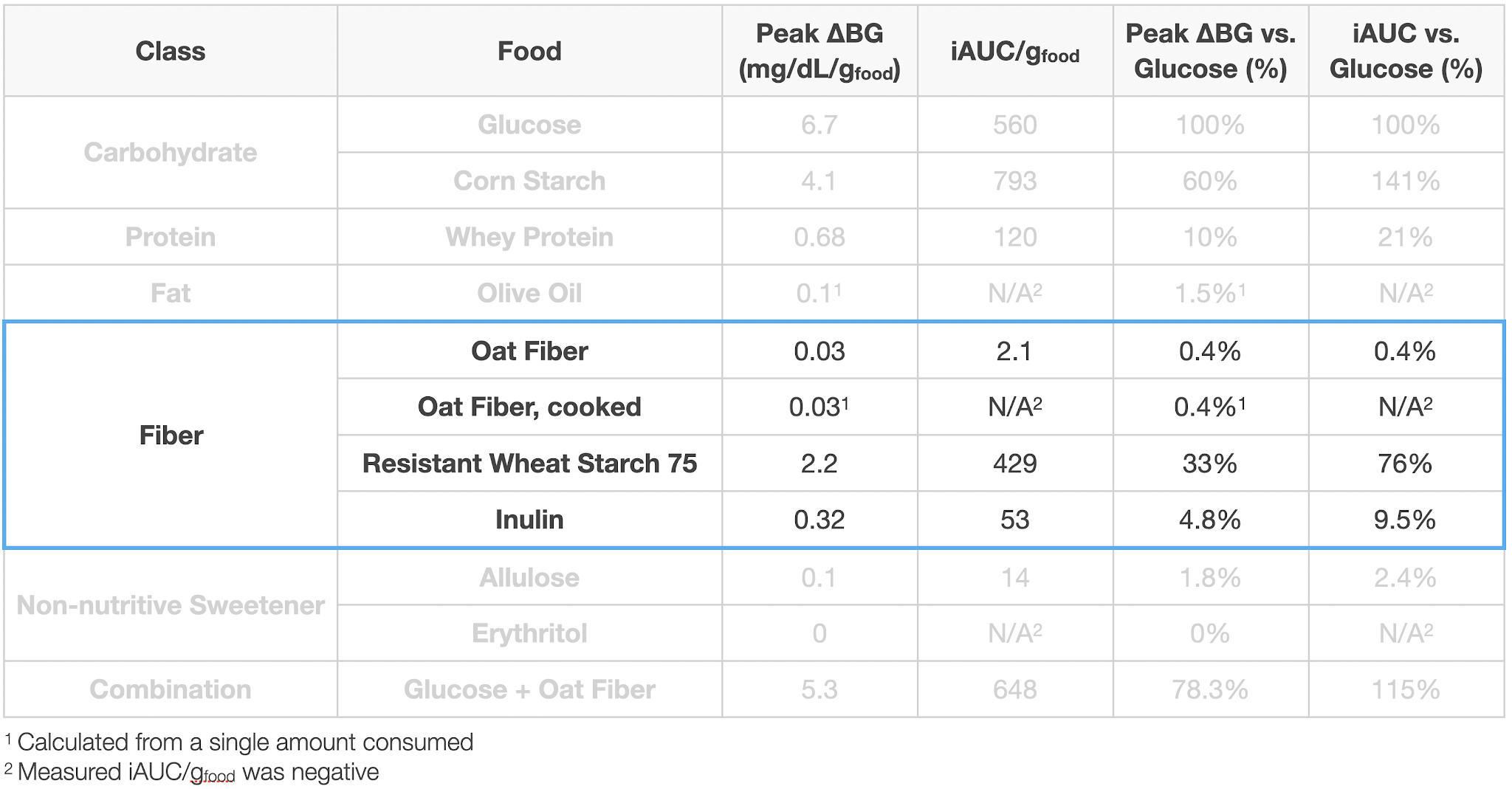
Insoluble or “indigestible” fiber had a wide range of impact, from near zero for oat fiber, ~10% of glucose for inulin, to 76% of glucose for resistant wheat starch.
This is extremely disconcerting, as both oat fiber (iAUC 0.4% of glucose) and resistant wheat starch (iAUC 75% of glucose) are listed as insoluble fiber on nutrition labels, but have radically different impact on blood sugar. Given the lack of clarity and quantification of ingredient lists, this makes it nearly impossible to predict the blood glucose impact of a food without eating it and testing.
My two preferred non-nutritive sweeteners, allulose and erythritol had negligible impact on my blood glucose.
Adding oat fiber to glucose had a negligible impact on blood glucose, though the time to peak was increased by 30 min. Further testing with different types of fiber and other macronutrients would be required to get a better handle on this effect, but the initial results suggest that while fiber might have an impact on rate of glucose absorption, it’s not signifiant enough to change the blood glucose impact for insulin-dependent diabetics (might be very different for someone who makes more endogenous insulin).
Details
Purpose
To quantify the effect of ingestion of food ingredients and ingredient combinations on my blood sugar.
Whey Protein. A complete protein extracted from milk whey. It’s the most popular protein supplement due to its ease of digestion, rapid absorption, and appreciable content of all 9 essential amino acids.
Olive Oil. A cooking oil that’s high in unsaturated fats, primarily oleic, linoleic, and palmitic acid. It’s used extensively in cooking.
Procedure. From 7 pm the day before through 4:30p the day of experiment, no food or calorie-containing drinks were consumed and no exercise was performed. Non-calorie-containing drinks were consumed as desired (water, caffeine-free tea, and decaffeinated coffee). At ~12 pm, the substance to be tested was dissolved or suspended in 475 mL of water and ingested as rapidly as comfortable. BGM measurements were then taken approximately every 15 min. for 2 h or until blood glucose had returned to baseline, whichever was longer. A final BGM measurement was taken 4.5 h after ingestion. Measurements. Blood glucose was measured using a FreeStyle Freedom Lite glucose meter with FreeStyle lancets & test strips. No special precautions were taken to clean the lancing site before measurement. To take a sample, the lancing devices was used to pierce the skin at an ~45° angle from the finger. Blood was then squeezed out by running the thumb and pointer finger of the opposite hand from the first knuckle to the lancing site of the finger. Blood was then wicked into a test strip that had been inserted into the meter and the glucose reading was recorded.
Data Processing & Visualization. iAUC was calculated using the trapezoid method (see data spreadsheet for details). Data was visualized using Tableau.
To determine the best time of day to measure the effect of food ingredients on my blood sugar, I monitored my blood sugar on three separate days while fasting. Based on the results, for all experiments in this study, I started fasting 7p the night before and started the measurement at 12p.
Glucose was used as the baseline for comparison for all other ingredients. It raises my blood sugar by 6.7 mg/dL/gglucose, with the peak occurring from 45-75 min. after ingestion. Results were extremely linear with amount consumed, with a slightly better fit when using incremental area under the curve (iAUC) vs. the peak increase (R2 = 0.988 vs. 0.983).
Corn starch had virtually the same effect as glucose, with an increase of 141% (by iAUC), but with a slower rise (110 vs. 76 min. for higher amounts consumed). This resulted in a slightly lower peak, 4.1 mg/dL/g(cornstarch) or 76% that of glucose.
Whey protein isolate increases my blood sugar by ~20% that of glucose (by iAUC), but with a slower rise. This result sin a lower peak, 0.68 mg/dL/g(whey) or 10% that of glucose, but a long tail of increased blood sugar, ~0.4 mg/dL/g(whey) @ 4.5 h.
Olive oil had a negligible effect on my blood sugar, ~0.1 mg/dL/g(olive oil) for ~350 kcal of oil, or 1.5% that of glucose.
This is mostly consistent with the medical literature. The two most interesting observations for me were:
Fat had virtually zero impact on my blood sugar. I’ve read a lot of posts and comments by people who dose a small amount of insulin based on the fat content of a meal. The claim is that it does increase their blood glucose, though much less than carbohydrates or proteins. My (limited) measurements do not show this.
If anyone reading this does see blood glucose rise with fat intake and is interested in doing a joint experiment to measure it, please let me know in the comments or send a PM via the contact form or to quantifieddiabetes_at_gmail.com.
Cornstarch had virtually the same impact on as glucose, just slightly delayed in time. Given the difference in their glycemic index (100 vs. 70), I would have expected a larger effect. That said, this suggests that for purposes of carbohydrate counting, I can treat all digestible carbohydrates the same.
Fiber was the most interesting and disturbing category. I looked at oat-fiber, resistant wheat starch, and inulin, all of which are claimed to be indigestible and have minimal impact on blood sugar (see ingredient backgrounds, above). Their actual impact on blood glucose, however, varied widely, ranging from near zero for oat fiber, ~10% of glucose for inulin, to 76% of glucose for resistant wheat starch.
This is extremely disconcerting, as both oat fiber (iAUC 0.4% of glucose) and resistant wheat starch (iAUC 75% of glucose) are listed as insoluble fiber on nutrition labels, but have radically different impact on blood sugar. Given the lack of clarity and quantification of ingredient lists, this makes it nearly impossible to predict the blood glucose impact of a food without eating it and testing.
The non-nutritive sweeteners I tried were a lot more promising. Both allulose and erythritol, my two favorite sweeteners, had negligible effect on my blood glucose up to the maximum quantity.
Glucose + Fiber
Many people claim that fiber can slow the absorption of sugar, helping to control blood sugar levels. Soluble fiber is generally claimed to have a stronger effect, but most soluble fibers are digestible and would contribute to blood sugar rise. Given that, I decided to test if oat fiber, and insoluble, indigestible fiber would slow blood sugar increase.
Towards that end, I tested glucose with an additional 44g of oat fiber. The impact on blood glucose was the same within the error of the measurement, but the time to peak was increased by 30 min. Further testing with different types of fiber and other macronutrients would be required to get a better handle on this effect, but the initial results suggest that while fiber might have an impact on rate of glucose absorption, it’s not signifiant enough to change the blood glucose impact for insulin-dependent diabetics (might be very different for someone who makes more endogenous insulin).
Final Thoughts & Next Experiments
Key results in the Summary section above.
Overall, the experiment was successful, yielding a reliable measure of the impact of the major macronutrients and my most commonly used low-carb ingredients. I also got preliminary insight into the interaction effect between glucose and insoluble fiber.
Due to external circumstances, I didn’t get to as many ingredients as I’d have liked. I may come back and do further experiments. I’m particularly interested in testing a wider range of purportedly low-carb ingredients and diving deeper into interaction effects (maybe looking foods with a range of different carbohydrate:protein:fat:fiber).
That said, these experiments were very time consuming and the frequent extended fasts were disruptive to my normal routine. I need to either find a simpler/easier experimental protocol or get more people to join in to accelerate data collection.
In the meantime, my plan for next experiments is:
Re-tune basal and bolus (meal) insulin doses
My routine has changed a lot due to working from home, changing doctors, and changing medication (due to insurance requirements). Plus, I was able to get a Dexcom G6 CGM, which is showing accuracy comparable to my blood glucose meter. Blood sugars are still good, but I think I can get them better.
Re-measure blood sugar impact of glucose and insulin; compare to previous data
While working from home, I’ve gained some weight (and hopefully muscle). This has resulted in a change in my insulin sensitivity. Not huge, but I need to remeasure to have an accurate baseline for future experiments.
Test the effect of some dietary supplements that have been reported to affect blood sugar in the literature, but where data insufficient or contradictory
Vitamin C (reported to cause blood glucose meters to read higher than actual, but all measurements I can find are for injected vitamin C)
Glutamate (reported to reduce post-prandial glucose, but magnitude and timing vary widely)
Others tbd.
As always, if you have any questions, comments, suggestions, or are interested in joining in future experiments, please let me know in the comments or send a PM via the contact form or to quantifieddiabetes_at_gmail.com.
As I mentioned in the previous post, my next set of experiments will be re-tuning my basal (background) and bolus (meal) insulin doses. Before I started that, I’d like to take a look at how my blood sugar has been over the last few months and lay out the plan for how I will adjust my insulin dosages.
Now that I’m using a Dexcom CGM, it’s much easier to monitor my blood sugar. From my own tests, after calibration my Dexcom matches my BGM (Freestyle Lite) within ~5 mg/dL, which is within the error of the meter, so I will just use the data from the Dexcom.
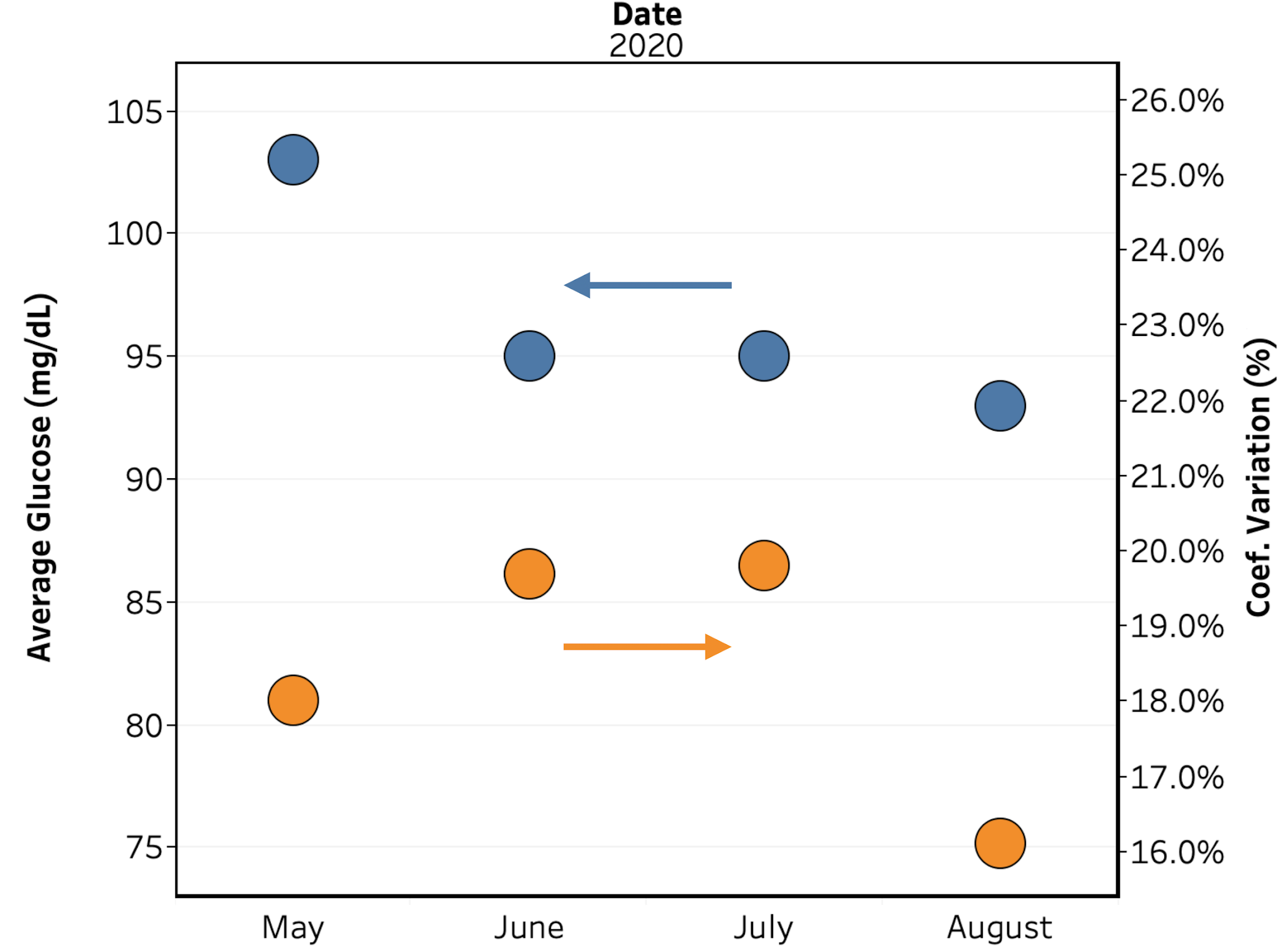
Dexcom provides a service, Clarity, that autogenerates reports based on your data. There’s a ton of options, but for my purposes, I’ll be looking at average blood glucose, coefficient of variation, and time in range.
Here’s the data broken out by month:
Figure 1.Average blood glucose (blue) & coefficient of variation (orange) by month.
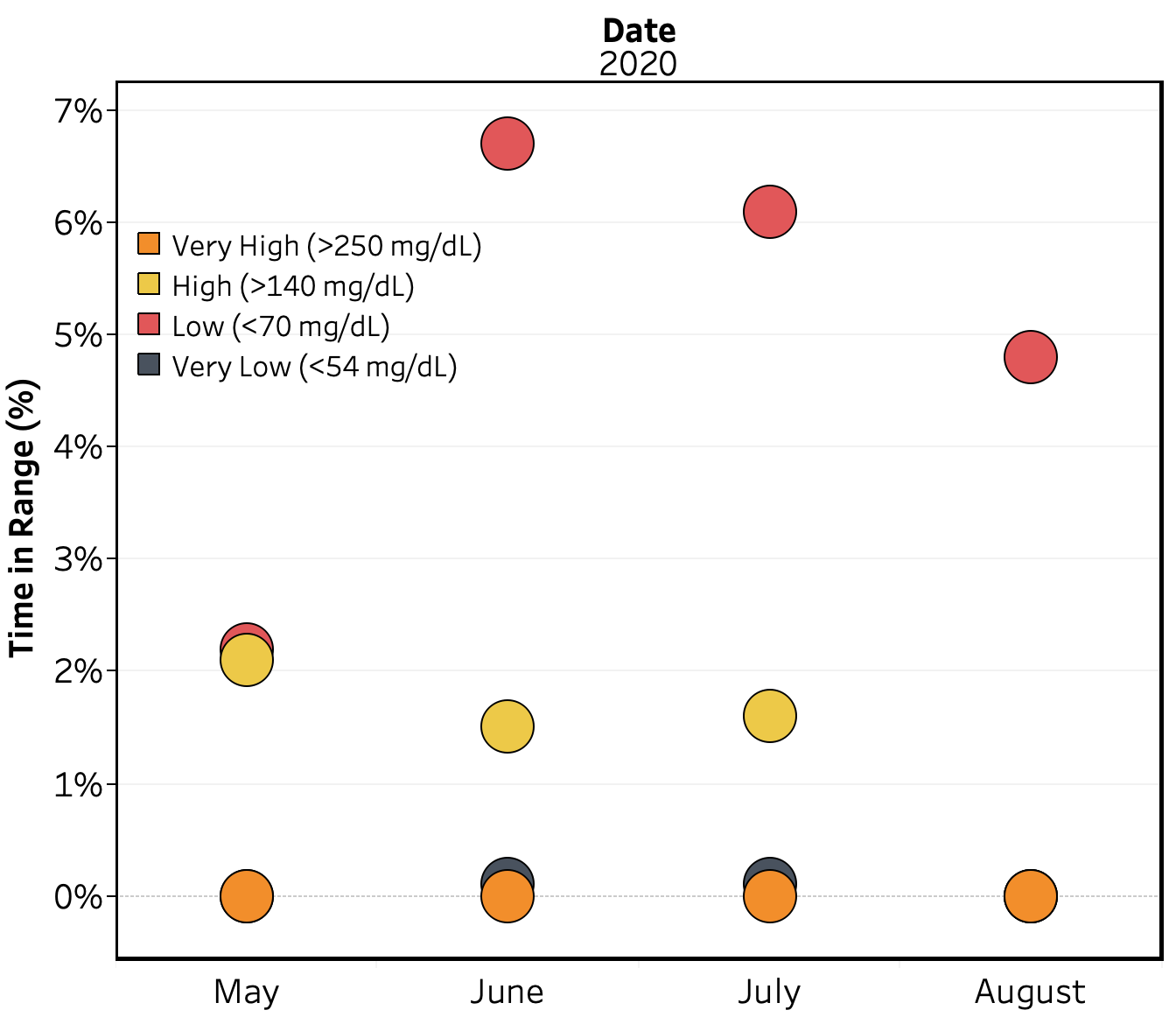
Figure 2. Time-in-range vs. month.
Figure 3. Time-in-range vs. month, excluding “in-range.”
Overall, my blood sugar is pretty good, but my time low is higher than I’d like. My suspicion is that this is due to my basal insulin being too high, resulting in me often going low between meals. Hopefully re-tuning my insulin doses will fix that.
To tune my insulin, I’m going to follow the approach described by Dr. Richard Bernstein in his book, Diabetes Solution, modified to use the vastly increased data from my CGM. I’ve used this in the past and it worked well for me. The basic procedure will be as follows:
Target an average blood sugar of 85 mg/dL.
Use my current insulin doses as baseline (Bernstein provides guidelines for how to estimate initial doses from scratch, but there’s no need for me to do that).
Adjust wait times between insulin injection and meals so that BG decreases by 5 mg/dL (to match timing of BG effect of insulin and food)
Adjust bolus insulin amount & type to minimize BG increase from the meal without causing an overall decrease in BG.
Adjust basal insulin amount to minimize BG change overnight and between meals
When I did this before, I was using a finger-stick meter and needed worth of data to make fine adjustments. I’m hoping that with the increased data quantity from the CGM, the process will go much faster. Finger’s crossed.
This self-experiment is being done as part of the Keating Memorial Self-Research Project. A couple of other people from the Open Humans community are also running the same experiments. If you’re interested in joining in, let me know in the comments or send me a PM.
This post is an update on my experiments measuring the effect of food ingredients on blood sugar.
This is especially problematic for predicting the blood glucose impact of foods from their nutrition information as based on my data so far, even insoluble fibers can range in impact from 0.4 – 76% of glucose.
Next week I’ll finish out the major macronutrient groups with cornstarch. Still deciding where to go after that, but it will either be more ingredients used in low carb cooking (inulin, erythritol, soluble corn fiber, lupin flour) or mixtures of the major macronutrients (to measure combinations effects.
Details
Purpose
To quantify the effect of ingestion of food ingredients and ingredient combinations on my blood sugar.
Procedure. From 7 pm the day before through 4:30p the day of experiment, no food or calorie-containing drinks were consumed and no exercise was performed. Non-calorie-containing drinks were consumed as desired (water, caffeine-free tea, and decaffeinated coffee). At ~12 pm, the substance to be tested was dissolved or suspended in 475 mL of water and ingested as rapidly as comfortable. BGM measurements were then taken approximately every 15 min. for 2 h or until blood glucose had returned to baseline, whichever was longer. A final BGM measurement was taken 4.5 h after ingestion.
Measurements. Blood glucose was measured using a FreeStyle Libre flash glucose monitor and a FreeStyle Freedom Lite glucose meter with FreeStyle lancets & test strips. No special precautions were taken to clean the lancing site before measurement. To take a sample, the lancing devices was used to pierce the skin at an ~45 deg. angle from the finger. Blood was then squeezed out by running the thumb and pointer finger of the opposite hand from the first knuckle to the lancing site of the finger. Blood was then wicked into a test strip that had been inserted into the meter and the glucose reading was recorded.
Data Processing & Visualization. iAUC was calculated using the trapezoid method (see data spreadsheet for details). Data was visualized using Tableau.
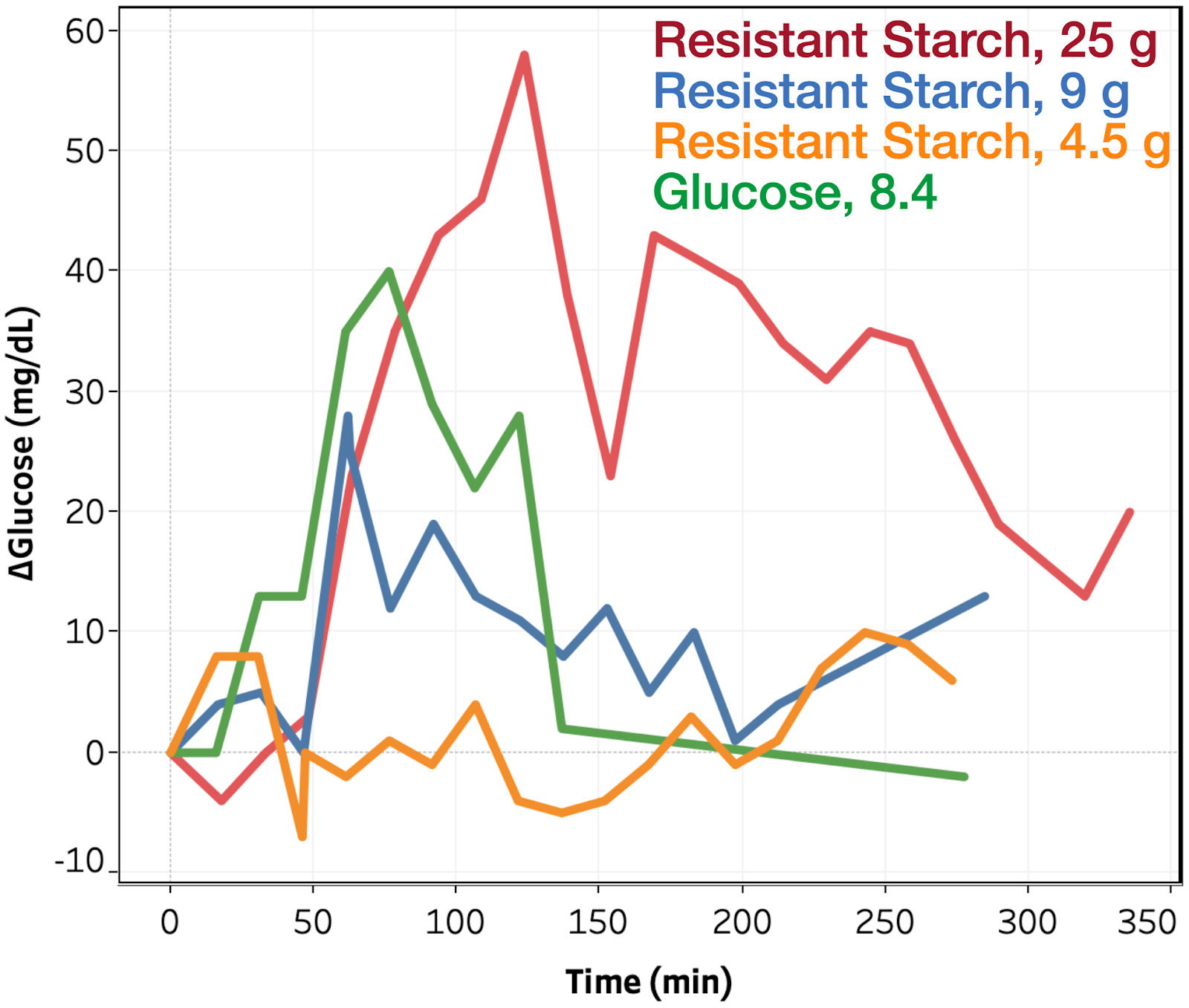
Figure 1. Change in blood glucose vs. time for resistant starch and glucose tests.
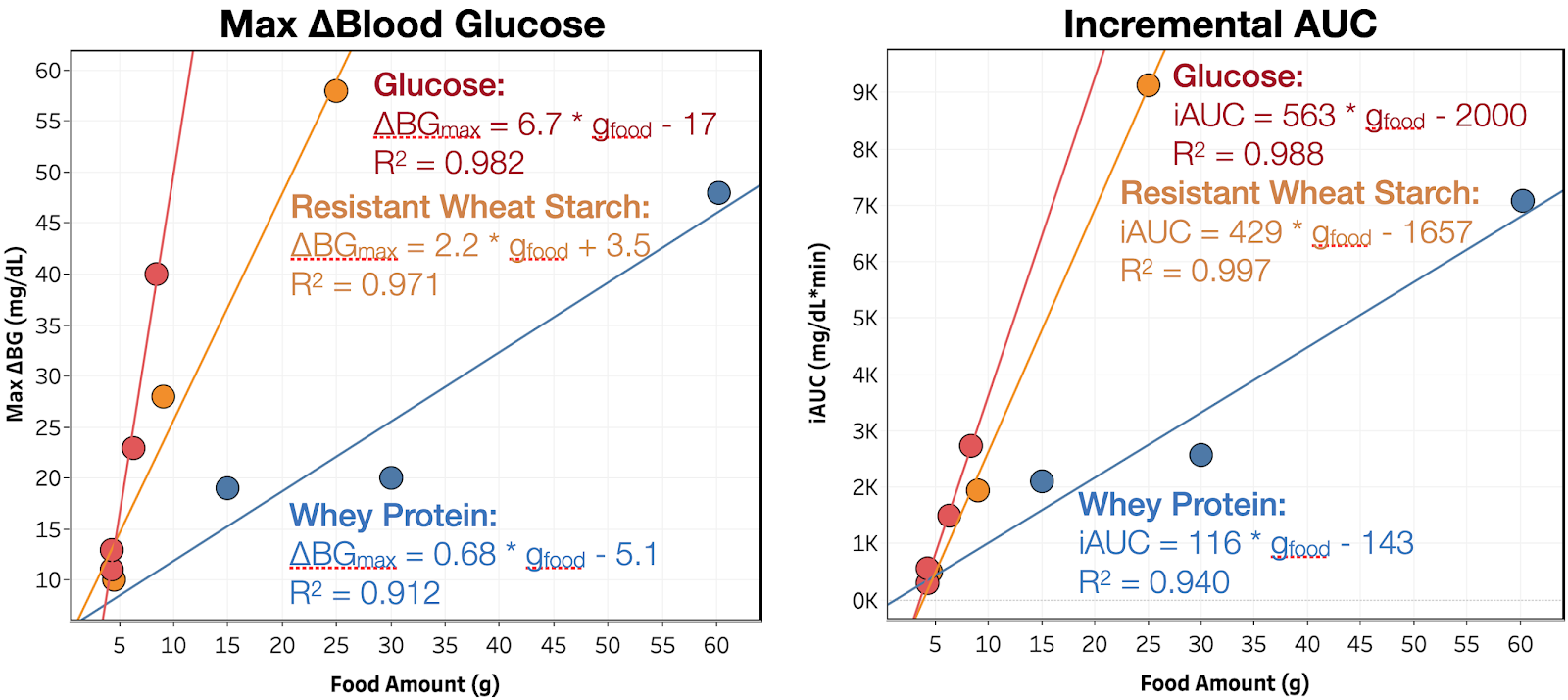
Figure 2. Maximum blood glucose increase and iAUC vs. amount consumed. Red, orange, and blue indicate glucose, resistant wheat starch, and whey protein isolate, respectively. Lines are the best linear fit to the data.
Changes in blood glucose as a function of time for the resistant wheat starch and glucose tests are shown in Figure 1. For resistant wheat starch, I observe an increase in blood glucose starting at ~45 min. and reaching a peak between 75-120 min. While the timing is similar to that of whey protein, the magnitude of impact is much larger, with the peak change in blood glucose and iAUC increasing by 33% and 76% vs. glucose. It will be interesting to see next week how regular corn starch compares to resistant wheat starch and therefore if the chemical modifications to resist digestion are having any meaningful impact.
Put together, this indicates that resistant wheat starch is slower to digest than glucose, but contrary to the claims above, is clearly still metabolized to glucose. This is extremely disconcerting, as both oat fiber (iAUC 0.4% of glucose) and resistant wheat starch (iAUC 75% of glucose) are listed as insoluble fiber on nutrition labels, but have radically different impact on blood sugar. Given the lack of clarity and quantification of ingredient lists, this makes it nearly impossible to predict the blood glucose impact of a food without eating it and testing.
Next week I’ll finish out the major macronutrient groups with cornstarch. Still deciding where to go after that, but it will either be more ingredients used in low carb cooking (inulin, erythritol, soluble corn fiber, lupin flour) or mixtures of the major macronutrients (to measure combinations effects.
This self-experiment is being done as part of the Keating Memorial Self-Research Project. A couple of other people from the Open Humans community are also running the same experiments. If you’re interested in joining in, let me know in the comments or send me a PM.
This post is an update on my experiments measuring the effect of food ingredients on blood sugar.
This week, I have the results from whey protein and olive oil.
Summary
Olive oil had a negligible effect on my blood sugar, ~0.1 mg/dL/g(olive oil) for ~350 kcal of oil, or 1.5% that of glucose.
Whey protein isolate increases my blood sugar by ~20% that of glucose (by iAUC), but with a slower rise. This result sin a lower peak, 0.68 mg/dL/g(whey) or 10% that of glucose, but a long tail of increased blood sugar, ~0.4 mg/dL/g(whey) @ 4.5 h.
Still deciding what to try next, but it will either be corn starch (to have an example from each major macronutrient), resistant starch (fiber with disputed claims to non-digestibility), or combinations of protein, fat, or fiber with sugar.
Details
Purpose
To quantify the effect of ingestion of food ingredients and ingredient combinations on my blood sugar.
Ingredient Background
Whey protein isolate is a complete protein extracted from milk whey. It’s the most popular protein supplement due to its ease of digestion, rapid absorption, and appreciable content of all 9 essential amino acids.
Olive oil is a cooking oil that’s high in unsaturated fats, primarily oleic, linoleic, and palmitic acid. It’s used extensively in cooking.
Design/Methods
Procedure. From 7 pm the day before through 4:30p the day of experiment, no food or calorie-containing drinks were consumed and no exercise was performed. Non-calorie-containing drinks were consumed as desired (water, caffeine-free tea, and decaffeinated coffee). At ~12 pm, the substance to be tested was dissolved or suspended in 475 mL of water and ingested as rapidly as comfortable. BGM measurements were then taken approximately every 15 min. for 2 h or until blood glucose had returned to baseline, whichever was longer. A final BGM measurement was taken 4.5 h after ingestion.
Measurements. Blood glucose was measured using a FreeStyle Libre flash glucose monitor and a FreeStyle Freedom Lite glucose meter with FreeStyle lancets & test strips. No special precautions were taken to clean the lancing site before measurement. To take a sample, the lancing devices was used to pierce the skin at an ~45 deg. angle from the finger. Blood was then squeezed out by running the thumb and pointer finger of the opposite hand from the first knuckle to the lancing site of the finger. Blood was then wicked into a test strip that had been inserted into the meter and the glucose reading was recorded.
Data Processing & Visualization. iAUC was calculated using the trapezoid method (see data spreadsheet for details). Data was visualized using Tableau.
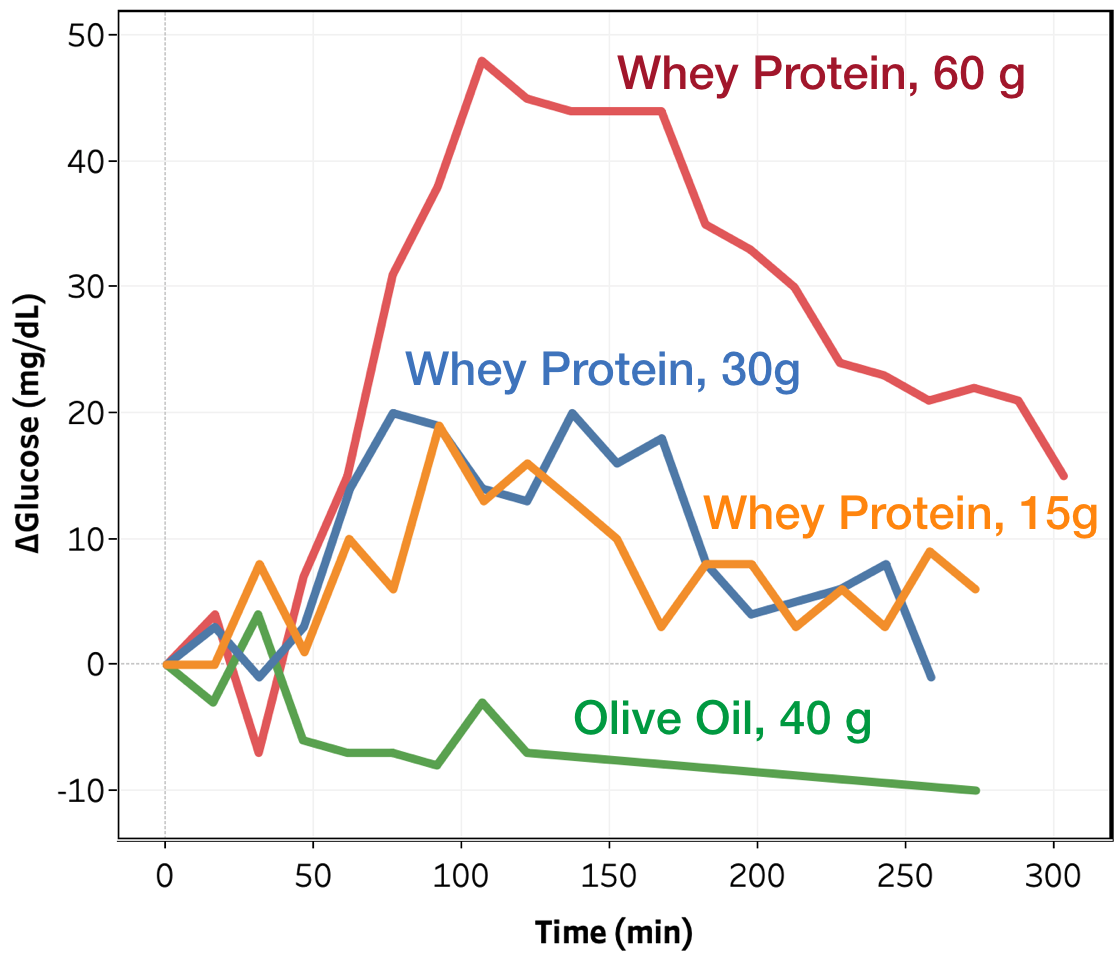
Figure 1. Change in blood glucose vs. time for whey protein and olive oil tests.
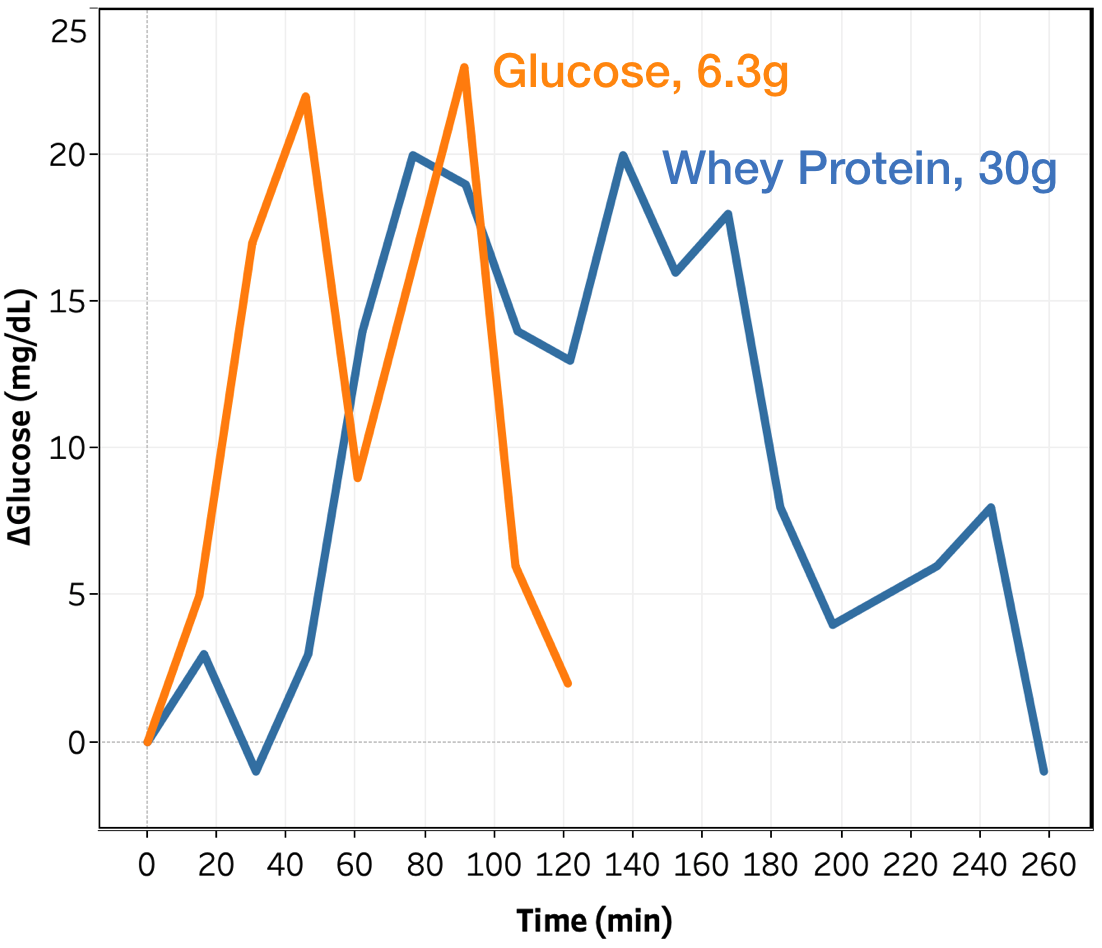
Figure 2. Change in blood glucose vs. time for whey protein and glucose for conditions with a peak of 20-25 Δmg/dL.
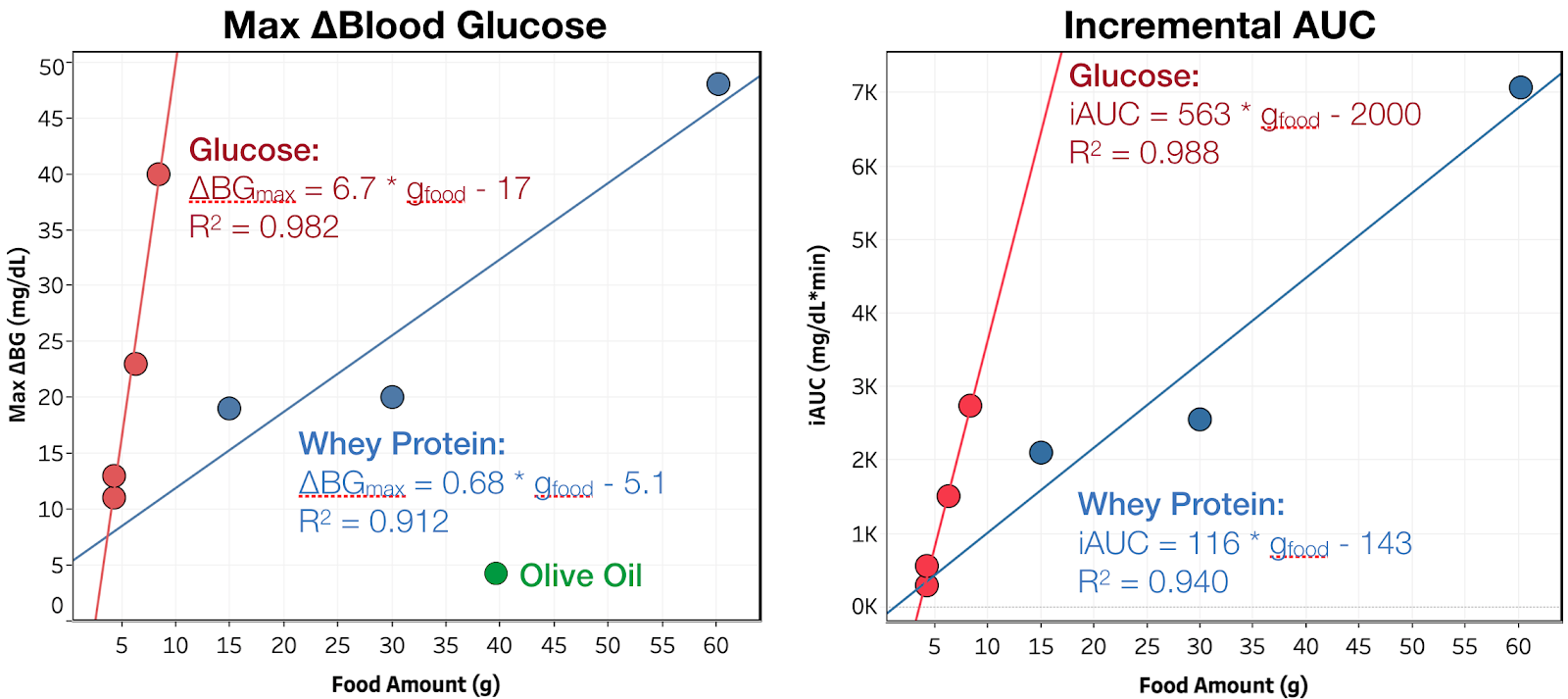
Figure 3. Maximum blood glucose increase and iAUC vs. amount consumed. Red, blue, and green indicate glucose, whey protein isolate, and olive oil, respectively. Lines are the best linear fit to the data.
Changes in blood glucose as a function of time for the whey protein isolate and olive oil tests are shown in Figure 1. As expected, olive oil showed no measurable impact on blood glucose at 40 g, or 350 kCal, consumed. Future experiments will look at whether it or similar oils can modulate the blood sugar response to ingredients that do impact blood sugar.
For whey protein, I observe an increase in blood glucose starting at ~45 min. and reaching a peak between 75-105 min. The magnitude increases with increasing amount consumed, but non-linearly; the difference between the 15 and 30 g consumed conditions is quite small. More data is needed at lower amounts consumed to see if this is a real effect or just noise in the data.
Comparing directly to glucose, for the same peak change in blood glucose, whey protein is much slower to impact my blood glucose and is metabolized over a much longer period of time. For example, looking at the conditions where peak Δmg/dL = 20-25 (see Figure 2):
Time to >5 mg/dL rise is 60 vs. 15 min. for whey vs. glucose
Time to return to <5 Δmg/dL is 255 vs. 120 min. for whey vs. glucose
Results are similar for all other amounts consumed. As show in Figure 3 and the summary table, this slower metabolism results in whey protein having a larger relative impact on iAUC than peak change in blood glucose (20 vs. 10% of glucose per gram). This may be do to giving my body more time to produce endogenous insulin, or even directly stimulating its production, reducing the peak blood glucose. Both of these effects have been reported. Given that, it would be useful to see the same measurements in someone with Type 1 diabetes, who does not produce endogenous insulin.
Conclusion & Next Experiments
Olive oil had a negligible effect on my blood sugar, ~0.1 mg/dL/g(olive oil) for ~350 kcal of oil, or 1.5% that of glucose.
Whey protein isolate increases my blood sugar by ~20% that of glucose (by iAUC), but with a slower rise. This result sin a lower peak, 0.68 mg/dL/g(whey) or 10% that of glucose, but a long tail of increased blood sugar, ~0.4 mg/dL/g(whey) @ 4.5 h.
Still deciding what to try next week, but it will either be corn starch (to have an example from each major macronutrient), resistant starch (fiber with disputed claims to non-digestibility), or combinations of protein, fat, or fiber with sugar.