Growing up, one of my favorite holiday dishes was my aunts French toast rolls, cream cheese filled rolls with a crispy, cinnamon sugar coating. No matter how many she made, they were always gone by the end of the night.
Just last week, I ran across a similar recipe on Food52, Pati Jinich’s French toast rolls (youtube, print). The main difference between the two was that my aunt’s recipe was baked and used a butter-based coating, while the Food52 version was pan-fried and used an egg & milk based coating.
Both sounded great, so I decided to compete them against each other.
The first step was to modify the recipes to be low-carb. To do that, I made the following changes:
Changed the cinnamon:sugar ratio to 1:4 (I prefer a stronger cinnamon taste)
Increased baking temperature to 400 °F to get a crispier outer layer.
Then I made the recipes, using the same batch of cream cheese filling (full recipe below). Both turned out fantastic. The sweetened cream cheese contrasts really nicely with the slightly savory bread and then the layer of crispy/sweet/cinnamon outer layer.
Detailed notes
Cooking:
The most labor intensive step was flattening the bread. Both recipes call for using a rolling pin, but I think a grill press would be a lot faster.
I overfilled the cream cheese, which led to some of the rolls unraveling during cooking. Still tasted good, but not as visually appealing. You really need only a thin layer of cream cheese (2-3 mm).
Low carb bread doesn’t absorb liquid as fast as regular bread. To adjust, just dip longer.
Convenience:
Both recipes were fairly easy to make, but the Food52 recipe cooks faster (~5 min. in the pan), while my family recipe is less labor intensive, especially in large quantities (~15 min. in the oven, but you can bake a lot at once).
My family recipe can be frozen before cooking, so you can make it ahead of time and then just bake right before serving. I tried this and it tasted exactly the same as fresh.
Taste & Texture:
The two recipes are similar, but my family recipe adds the cinnamon sugar before cooking, giving it a more intense flavor and a crispier texture.
Overall, I significantly prefer the family recipe, both for taste and convenience, which I’m sure will make my aunt happy.
The winner! Zoomed in because they look great.
I’ve included both recipes below if you want to try them yourself.
Hope you enjoy it!
– QD
Low-Carb French Toast Rolls (Stovetop & Oven Baked)
Trim the crust from the bread and flatten with a rolling pin or grill press.
Mix sugar, cream cheese, and vanilla until homogeneous.
Spread ~1 tsp. of filling on each bread slice, roll tightly into a cylinder, cut in half, and set aside.
Mix together allulose and cinnamon to make the cinnamon “sugar.”
Stovetop
Whisk together egg, almond milk, vanilla, and salt.
Melt buter in a skillet over medium heat. Soak the rolls in the milk mixture until fully coated, add to the skillet, and cook until golden brown on all sides.
Toss each roll in the cinnamon mixture and serve warm.
Oven Baked
Heat oven to 400 °F.
Dip each roll in the melted butter, then roll in the cinnamon mixture. Rolls can be frozen at this stage until ready to bake.
Bake for 12-15 min., until heated through and browned.
Notes
0.7g net carbs per roll.
Nutrition information calculated for the oven baked recipe by adding up macros of the individual ingredients. Stovetop recipe is ~60 cal and 3.8g fat/roll, same carb and protein count.
This self-experiment is being done as part of the Keating Memorial Self-Research Project. A couple of other people from the Open Humans community are also running the same experiments. If you’re interested in joining in, let me know in the comments or send me a PM.
This post is an update on my experiments measuring the effect of food ingredients on blood sugar.
This week, I have the results from oat fiber and got started on whey protein.
Summary
Oat fiber has a negligible effect on my blood sugar, <0.05 mg/dL/g(oat fiber), or <0.5% that of glucose. Cooking the oat fiber had no significant effect. So, I’m safe to keep baking with it ☺.
Details
Purpose
To quantify the effect of ingestion of food ingredients and ingredient combinations on my blood sugar.
Procedure. From 7 pm the day before through 4:30p the day of experiment, no food or calorie-containing drinks were consumed and no exercise was performed. Non-calorie-containing drinks were consumed as desired (water, caffeine-free tea, and decaffeinated coffee). At ~12 pm, the substance to be tested was dissolved or suspended in 475 mL of water and ingested as rapidly as comfortable. For the cooked oat fiber, 100 g oat fiber was mixed with 200 g water and allowed to hydrate for 30 min. The mixture was then baked in a parchment lined muffin tin for 18 min. at 350 °F. The oat fiber was then suspended as described above. BGM measurements were then taken approximately every 15 min. for 2 h or until blood glucose had returned to baseline, whichever was longer. A final BGM measurement was taken 4.5 h after ingestion.
Measurements. Blood glucose was measured using a FreeStyle Libre flash glucose monitor and a FreeStyle Freedom Lite glucose meter with FreeStyle lancets & test strips. No special precautions were taken to clean the lancing site before measurement. To take a sample, the lancing devices was used to pierce the skin at an ~45 deg. angle from the finger. Blood was then squeezed out by running the thumb and pointer finger of the opposite hand from the first knuckle to the lancing site of the finger. Blood was then wicked into a test strip that had been inserted into the meter and the glucose reading was recorded.
Data Processing & Visualization. iAUC was calculated using the trapezoid method (see data spreadsheet for details). Data was visualized using Tableau.
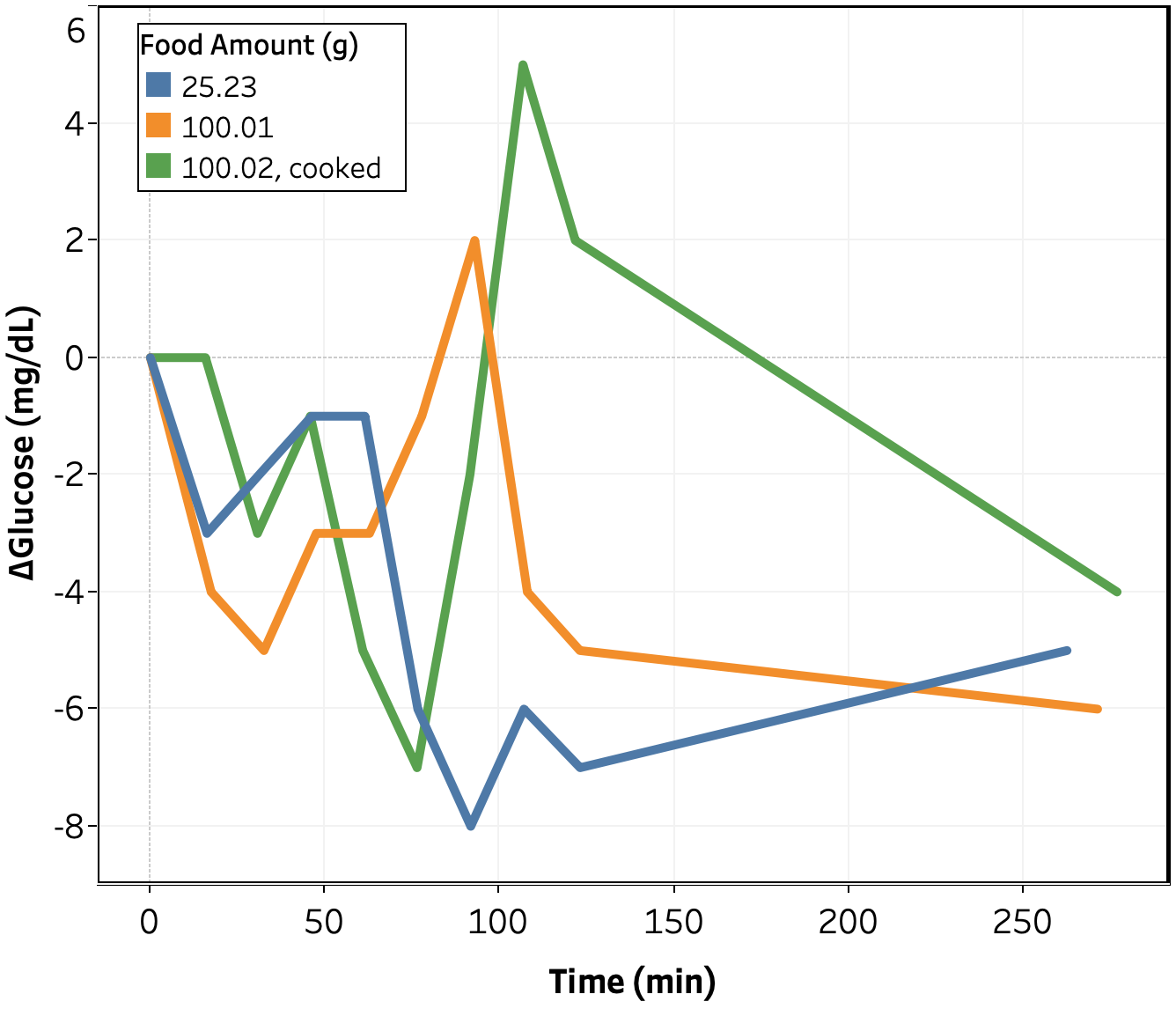
Figure 1. Change in blood glucose vs. time for oat fiber tests.
Change in blood glucose as a function of time for the oat fiber tests is shown in Figure 1. Qualitatively, there appears to be no impact of oat fiber up to 100 g consumed. It was extremely uncomfortable to drink that much oat fiber in one sitting, so it’s unlikely I will ever eat more than that.
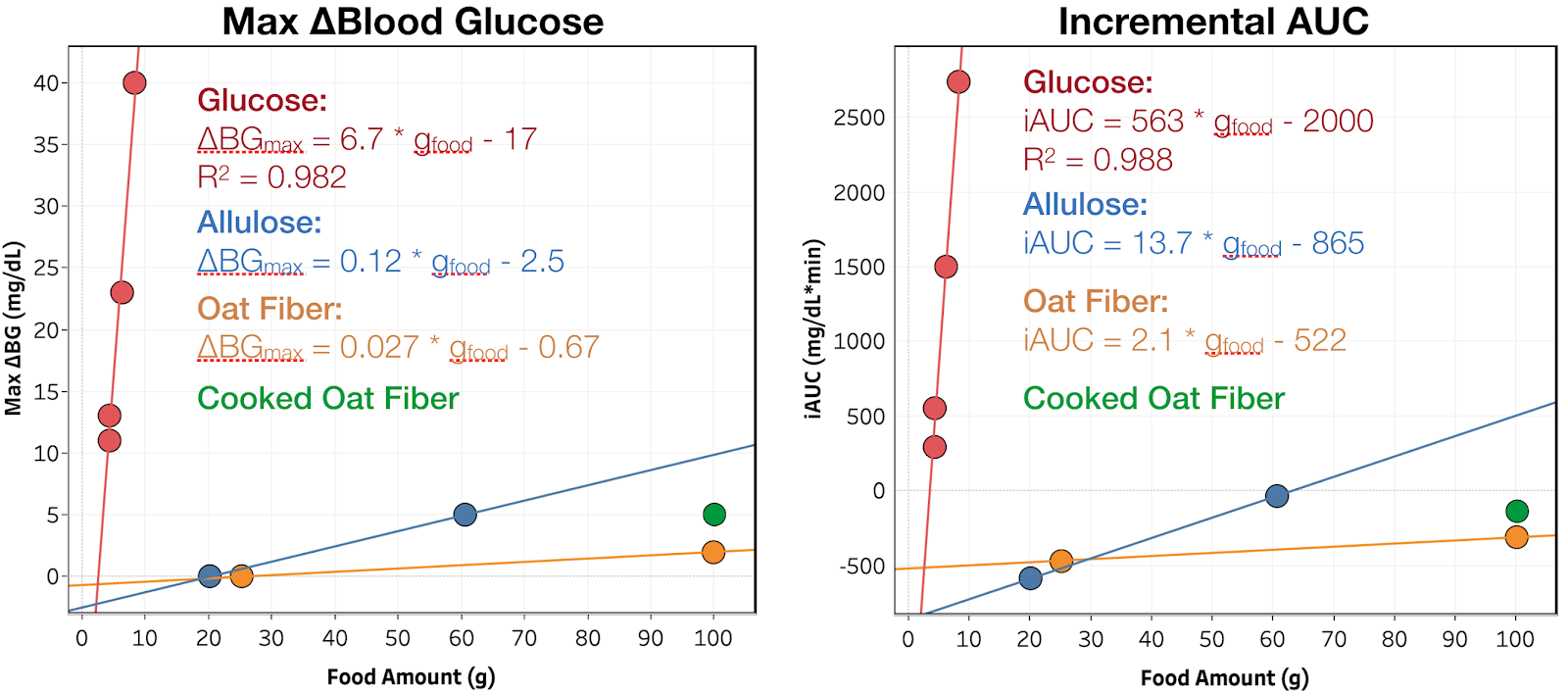
Figure 2. Maximum blood glucose increase and iAUC vs. amount consumed. Red, blue, orange, and green indicate glucose, allulose, oat fiber, and cooked oat fiber, respectively. The line is the best linear fit to the data.
To better quantify the impact of glucose on my blood glucose, I plotted the maximum increase in blood glucose and the iAUC of blood glucose (incremental area under the curve) vs. amount consumed for all ingredients tested so far (see Figure 2). While the oat fiber data shows an increase in both blood glucose and iAUC as a function of amount consumed, there’s only two data points and the magnitude is extremely small and could easily be due to experimental error. Confirming this effect would require running more measurements. I may go back and do this later, but for the moment, I would prefer to focus my time on ingredients with unknown or more substantial effects.
Since oat fiber is used in baking, I also wanted to check if heating it would break down the fibers and increase digestibility. Towards that end, I mixed 100 g of oat fiber with 200 g of water and baked at 350 °F for 18 min. (time & temperature for my muffin recipe and longer than my cookie recipe), then suspended it in water using the same procedure as with the uncooked fiber. There was no observable change in appearance, taste, or texture from the cooking process. There was a very minor increase in blood glucose response, but well within the measurement error of the meter.
Conclusion & Next Experiments
Oat fiber has a negligible effect on my blood sugar, <0.05 mg/dL/g(oat fiber), or <0.5% that of glucose. Cooking the oat fiber had no significant effect. This week, I will measure the effect of whey protein, a common protein supplement.
Following up on my French Toast post, I wanted to try find a good zero-carb maple syrup to go along with it. On Reddit, u/botrock22 recommended All-u-Lose; I also found several other brands on Amazon that looked pretty good. I also did a search for low-carb or keto maple syrup recipes and found a couple that looked promising.
To figure out which I liked best, I decided to do a taste test.
My versions, adapted from Mel’s Kitchen with the following modifications:
All: allulose + 5g molasses substituted for white & brown sugars, maple extract increased 4x
Version 1: 120 g water (33 wt%)
Version 2: 80 g water (24 wt%)
Version 3: 50 g water (17 wt%)
I assessed each syrup on the following factors:
Calories
Net carbs
Ingredients
Cost
Taste
Texture
Here’s the results:
Note: After I bought it, I noticed the Sweet-Like-Syrup brand uses isomaltose as the sweetener. Isomaltose is not low carb (GI = 35), so I didn’t try it.
For me, homemade version #2 (24 wt% water) was the clear winner, probably because it was adjusted to my taste preference. It had a strong maple flavor, was thick enough to cling to the french toast while still spreading easily, and didn’t have any unpleasant aftertaste. It was also extremely easy to make and cheaper to boot. I’m going to start keeping a batch around for French toast, pancakes, and other deserts.
I’ve included the recipe below if you want to make it yourself.
This post is the final report on our Community Self-Experiment studying the effect of hot showers on blood glucose. If you don’t want to read all the details, the highlights are in the Background & Summary section immediately below.
To figure out what’s really going on, we decided to do a communal self-experiment. 8 Redditors with diabetes developed an experimental protocol, measured their blood glucose before and after 41 showers using a combination of CGMs and BGMs, and analyzed the results.
Summary of Results
By working together, the team of experimenters was able to learn more and learn faster than any one of us would have been able to on our own. From the data, we were able to answer several of our initial questions:
What is the change in blood glucose after a hot shower under controlled conditions?
From BGM: 12 ± 17 mg/dL
From CGM: 21 ± 15 mg/dL
Is the observed change in blood glucose real or a CGM sensor artifact?
The change is real, not a sensor artifact (change is observed with BGM; CGM measurements are consistent with typical variation between CGM and BGM)
We cannot rule out the difference in effect size between BGM and CGM being due to a sensor artifact, but the data does not provide support for this hypothesis.
Is there significant person-to-person variation in the magnitude or direction of the effect?
The data is consistent with person-to-person variation, but significantly more data and/or more controlled conditions are required to determine if the variation exists and it’s effect size.
Is the change in blood glucose cause by the hot shower?
We can not identify any factors that account for the blood glucose rise other than the shower, but would need significantly more data and/or more controlled conditions to be certain that the shower is the cause.
While we were not able to get firm answers to all of our questions, we did get a measure of the effect size and rule out it being a CGM sensor artifact (the leading hypothesis in the original post). We also learned a lot that will help guide future Community Self-Experiments.
Data Processing. All data was converted into consistent units and put into an excel spreadsheet. From the raw data, I calculated change in BG from start of shower, as well as the largest relative change, and the time until largest relative change (see spreadsheet for calculation details). Visualization was done using Tableau.
What is the change in blood glucose after a hot shower under controlled conditions?
To answer this question, I plotted largest observed change over the 1 hour monitoring period for each shower as measured by both BGM and CGM (see Figure 1).
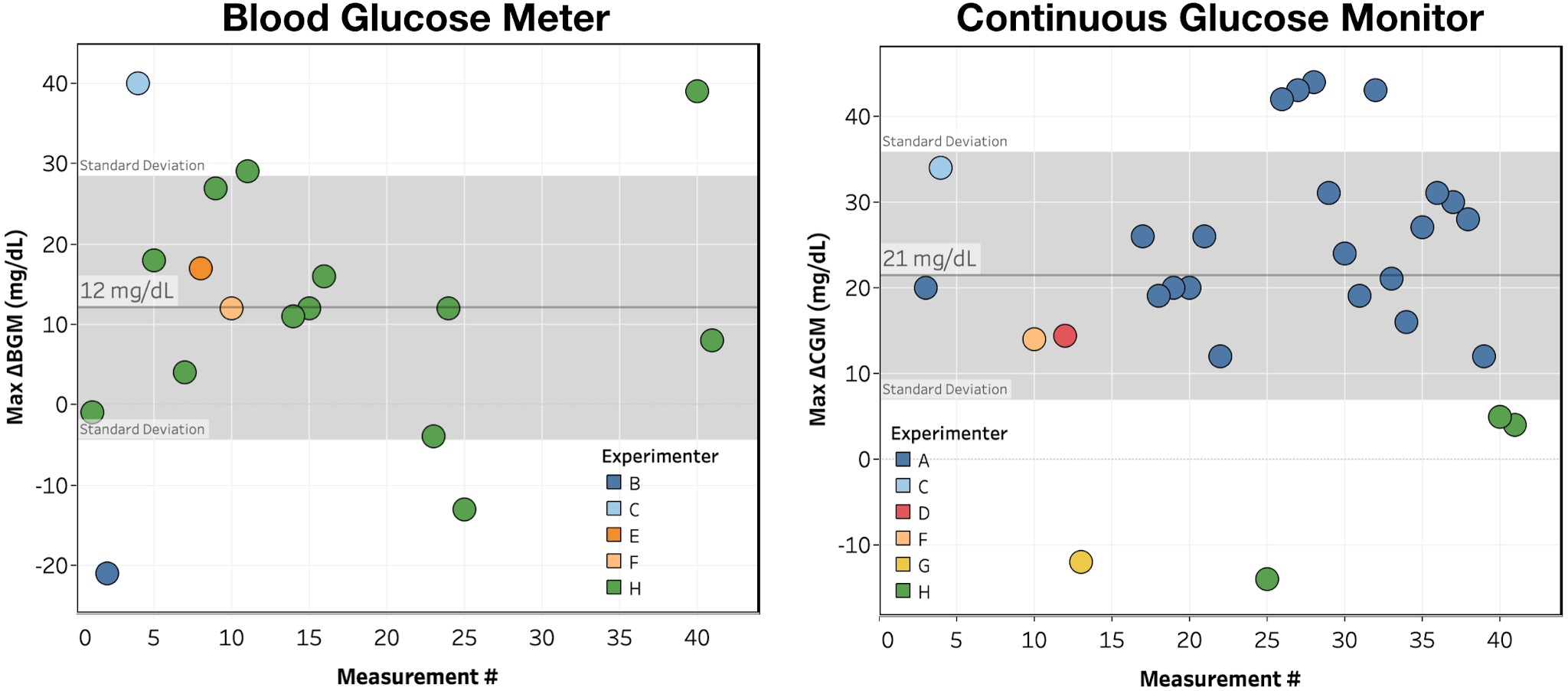
Figure 1. Max ΔBGM & ΔCGM for each shower, colored by experimenter. Reference band shows average +/- 1 standard deviation.
Looking at the data in Figure 1:
There is a large rise in blood glucose following a hot shower, though with significant variance in the size of the effect.
The rise is observed for both BGM (12 ± 17 mg/dL) and CGM (21 ± 15 mg/dL) measurements.
By count, we see (1 measurement excluded due to recording error):
>5 mg/dL increase: 34/40 (85%)
>5 mg/dL decrease: 3/40 (7.5%)
<5 mg/dL change: 3/40 (7.5%)
Conclusion: Blood glucose showed a consistent, measurable increase within 1h of taking a hot shower.
Is the observed change in blood glucose real or a CGM sensor artifact?
Looking again at Figure 1, the increase in blood glucose is seen for both BGM and CGM measurements, indicating that it can’t be just a CGM artifact.
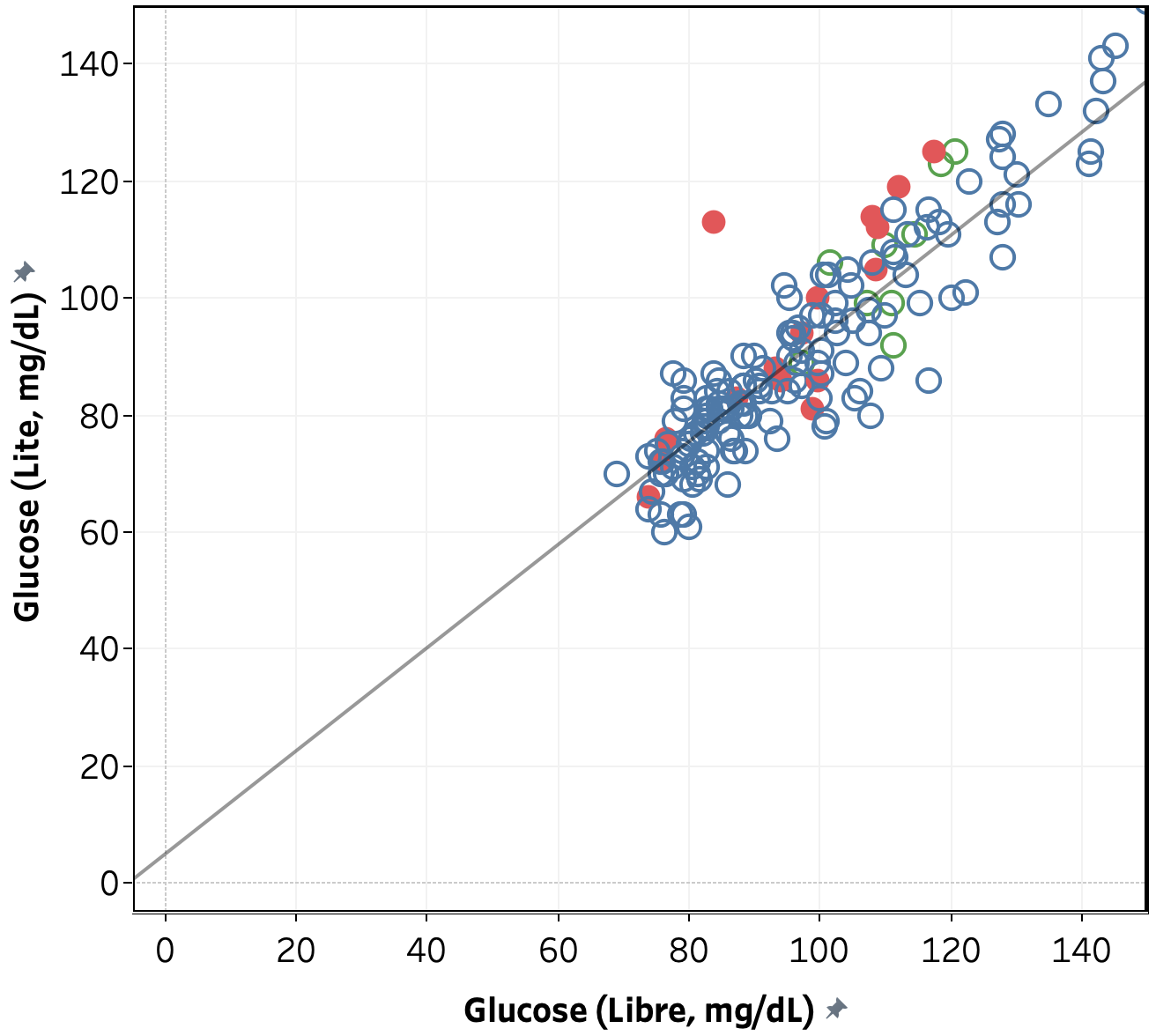
To further confirm this conclusion, we looked at the data from person H comparing BGM vs. CGM measurements during the normal course of the day vs. after a shower. As shown in Figure 2, for a single Libre sensor, there is a linear relationship between measured blood glucose by BGM vs. CGM and the data collected immediately and 15 minutes after a shower mostly lies within the normal variance in the data, with all exceptions showing a lower blood glucose measured by CGM. This indicates that any variation in CGM data due to a sensor artifact is smaller than the observed increase in blood glucose. Note that while this confirms that the measured effect is not exclusively due to a sensor artifact, it is still possible that a sensor artifact accounts for the difference in effect size as measured by BGM vs. CGM (12 vs. 21 mg/dL).
Figure 2. Blood glucose measured by FreeStyle Libre and FreeStyle Freedom Lite for person H over the course of 10 days. Grey line is a linear fit to the data and data collected immediately and 15 min. after a hot shower is shown in red.
Conclusion: The observed increase in blood glucose is not a CGM sensor artifact (though a partial effect from the CGM sensor is not ruled out).
Is there significant person-to-person variation in the magnitude or direction of the effect?
Looking again at the data in Figure 1:
A >5 mg/dL increase in blood sugar is observed for 6/8 (75%) of participants, with 2/8 (25%) showing a >5 mg/dL decrease in blood sugar.
Only 2 participants provided multiple measurements, A and H. For those we observe:
A: 12 ± 16 mg/dL
H: 26 ± 14 mg/dL
The difference is statistically significant (Welch’s t-test, p=0.016), but since the measurements were made using different methods (CGM for A, BGM for H), times (10 min. for A, 20 min. for H), and temperatures, this is only weak evidence for person-to-person variation.
Conclusion: The data is consistent with person-to-person variation, but significantly more data and/or more controlled conditions are required to determine if the variation exists and it’s effect size.
Is the change in blood glucose cause by the hot shower?
This is the most difficult question to answer. In hindsight, we should have done some randomized experiments where the experimenters held conditions as constant as possible, randomly decided whether or not to shower, and measured blood glucose either way. In the absence of that data, we analyzed the data we had for any correlation between the blood glucose rise and non-shower factors. It should be noted that the protocol did not control for any of these factors, so no causation or lack thereof should be inferred from the analysis.
Max ΔBGM or Max ΔCGM vs. hour of the day – no trend across the whole data set, nor within experimenters
Max ΔBGM vs. starting BGM – no trend across the whole data set, but within Experimenter H’s data, there’s an indication of a negative correlation (R2 = 0.32, p = 0.045).
Max ΔCGM vs. starting CGM – no clear trend across the whole data set, nor within experimenters.
Max ΔBGM vs. Temperature – no clear trend across the whole data set, nor within experimenters. Note: most experimenters did not record the shower temperature and the one who did (Person H) kept the temperature within ±3 °C.
Max ΔBGM or Max ΔCGM vs. Time since last meal or medication – There’s a positive correlation over the whole data set, but it doesn’t hold up within the two experimenters with repeat measurements, suggesting that it’s an effect person-to-person variation, possibly caused by systematic variation in conditions.
Conclusion: We can not identify any factors that account for the blood glucose rise other than the shower, but would need significantly more data and/or more controlled conditions to be certain that the shower is the cause.
Conclusions & Lessons Learned
By working together, the team of experimenters was able to learn more and learn faster than any one of us would have been able to on our own. From the data, we were able to answer several of our initial questions.
Conclusions:
What is the change in blood glucose after a hot shower under controlled conditions?
From BGM: 12 ± 17 mg/dL
From CGM: 21 ± 15 mg/dL
Is the observed change in blood glucose real or a CGM sensor artifact?
The change is real, not a sensor artifact (change is observed with BGM; CGM measurements are consistent with typical variation between CGM and BGM)
We cannot rule out the difference in effect size between BGM and CGM being due to a sensor artifact, but the data does not provide support for this hypothesis.
Is there significant person-to-person variation in the magnitude or direction of the effect?
The data is consistent with person-to-person variation, but significantly more data and/or more controlled conditions are required to determine if the variation exists and it’s effect size.
Is the change in blood glucose cause by the hot shower?
We can not identify any factors that account for the blood glucose rise other than the shower, but would need significantly more data and/or more controlled conditions to be certain that the shower is the cause.
While we were not able to get firm answers to all of our questions, we did get a measure of the effect size and rule out it being a CGM sensor artifact (the leading hypothesis in the original post). We also learned a lot that will help guide future Community Self-Experiments.
Key Lessons Learned:
Community Self-Experiments enable collection of data much faster than single-person experiments, both because more people are collecting data and because the group activity motivates participants.
Take more care with the experimental design, especially the implementation of control experiments to help rule out alternate hypotheses.
Implement better data sharing/management. In this experiment, data was posted, then manually entered into an excel sheet, which was very time consuming.
This self-experiment is being done as part of the Keating Memorial Self-Research Project. A couple of other people from the Open Humans community are also running the same experiments. If you’re interested in joining in, let me know in the comments or send me a PM.
This post is an update on my experiments measuring the effect of food ingredients on blood sugar.
Procedure. From 7 pm the day before through 4:30p the day of experiment, no food or calorie-containing drinks were consumed and no exercise was performed. Non-calorie-containing drinks were consumed as desired (water, caffeine-free tea, and decaffeinated coffee). At ~12 pm, the substance to be tested was dissolved or suspended in 475 mL of water and ingested as rapidly as comfortable. BGM measurements were then taken approximately every 15 min. for 2 h or until blood glucose had returned to baseline, whichever was longer. A final BGM measurement was taken 4.5 h after ingestion.
Measurements. Blood glucose was measured using a FreeStyle Libre flash glucose monitor and a FreeStyle Freedom Lite glucose meter with FreeStyle lancets & test strips. No special precautions were taken to clean the lancing site before measurement. To take a sample, the lancing devices was used to pierce the skin at an ~45 deg. angle from the finger. Blood was then squeezed out by running the thumb and pointer finger of the opposite hand from the first knuckle to the lancing site of the finger. Blood was then wicked into a test strip that had been inserted into the meter and the glucose reading was recorded.
Data Processing & Visualization. iAUC was calculated using the trapezoid method (see data spreadsheet for details). Data was visualized using Tableau.
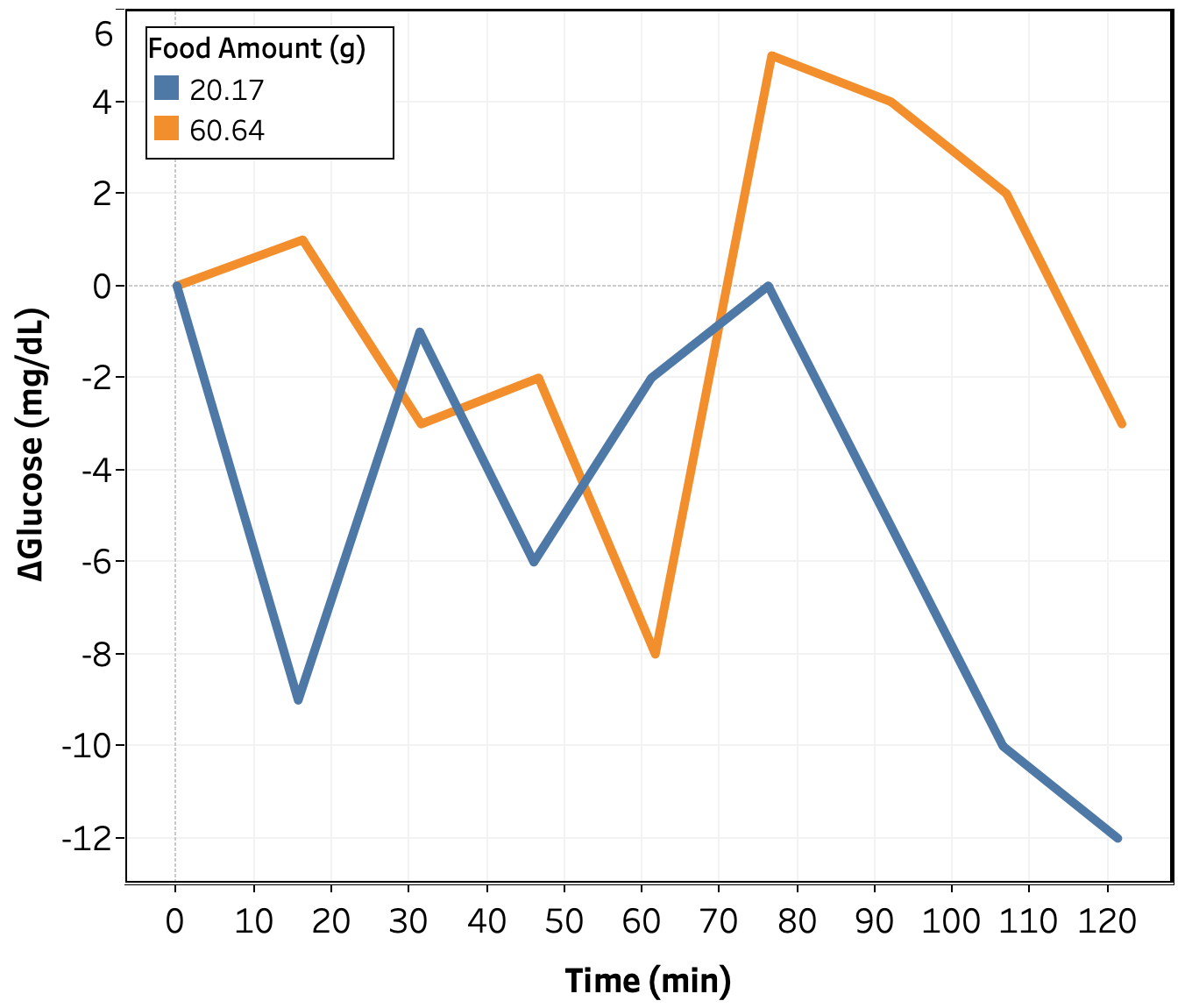
Figure 1. Change in blood glucose vs. time for alluose tests.
Change in blood glucose as a function of time for the allulose tests is shown in Figure 1. Qualitatively, there appears to be no impact of allulose up to 60 g consumed, with the possible exception of a small around 75 min.
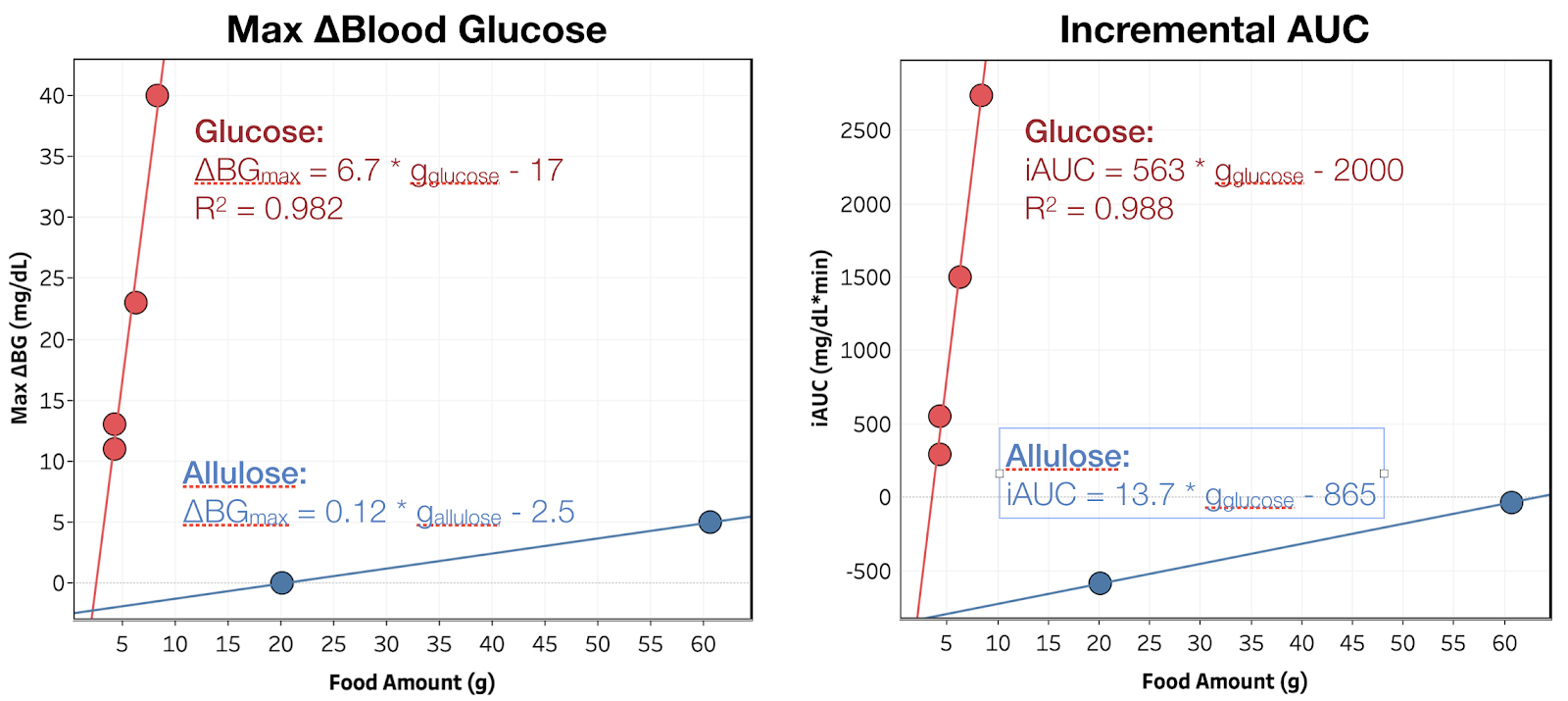
Figure 2. Maximum blood glucose increase and iAUC vs. amount consumed. Red and blue indicate glucose and allulose, respectively. The line is the best linear fit to the data.
To better quantify the impact of glucose on my blood glucose, I plotted the maximum increase in blood glucose and the iAUC of blood glucose (incremental area under the curve) vs. amount consumed for both glucose and allulose (see Figure 2). While the allulose data shows an increase in both blood glucose and iAUC as a function of amount consumed, there’s only two data points and the magnitude is extremely small and could easily be due to experimental error. Confirming this effect would require running more allulose measurements. I may go back and do this later, but for the moment, I would prefer to focus my time on ingredients with unknown or more substantial effects.
Lastly, I continue to observe a large negative intercept, suggesting a background drop in blood sugar during the experimental window.
Conclusion & Next Experiments
Allulose has a negligible effect on my blood sugar, <0.1 mg/dL/g(allulose), or <2% that of glucose. This week, I will measure the effect of oat fiber, a zero calorie, zero digestible carbohydrate flour replacement.